The 23,000 Unexplained Deaths in England and Wales That Raise Serious Questions of Vaccine Safety
NICK BOWLER for DAILY SCEPTIC

Can we find signals of vaccine injury deaths in U.K. mortality data? Will Jones isn’t sure, but I think we can.
A recent study by the Health Foundation at first glance suggests there is very little to cause concern. Indeed, the headline number of 34,000 fewer non-Covid deaths during the pandemic, together with the fact that non-Covid deaths have been lower than average during 80% of the period, should be a cause for some celebratory relief. However, this is not the end of the story, and there are some important caveats to this rather rosy outlook. A major one is the possibility that Covid deaths have been overcounted by Covid being ascribed to deaths from other causes, and non-Covid deaths correspondingly undercounted.
There has been some discussion of this in the media recently, and it is indeed a distinct possibility as the UKHSA definition of a Covid death is one that has occurred within 28 days of a positive Covid diagnosis, whether or not that person died for another reason. In the analysis below I am using ONS data, where the definition is that COVID-19 appears somewhere on the death certificate. This means it includes deaths where COVID-19 was not the underlying cause. There is also evidence that COVID-19 was put as underlying cause more often than it should have been. Insofar as Covid deaths have indeed been overcounted and non-Covid deaths undercounted, the trends presented here will be underestimates and the true trends will be larger.
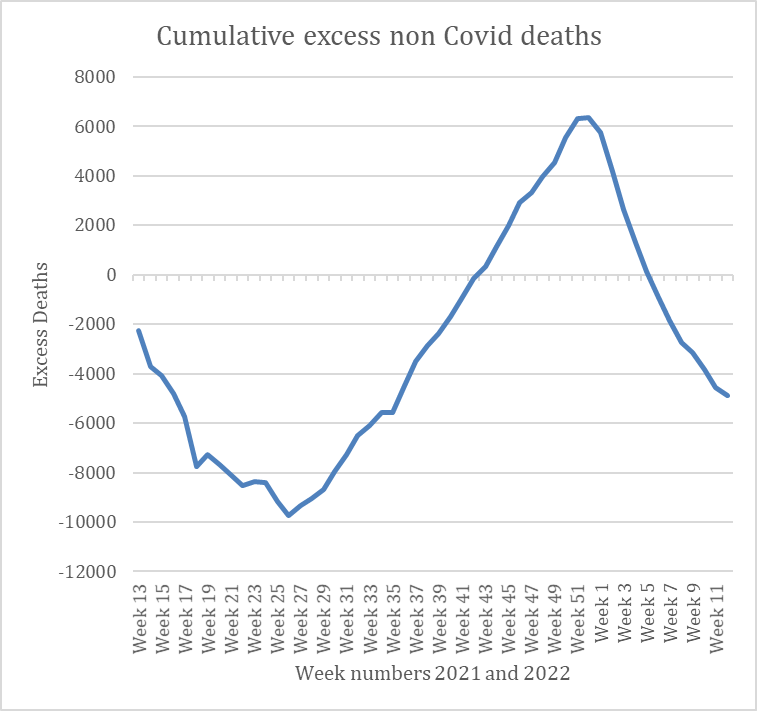
This is what a chart of the non-Covid mortality in England and Wales looks like for the period in question using the raw mortality data from the ONS, without any adjustments being applied. It might best be characterised as inconclusive.
However, the Health Foundation report does provide two major clues as to whether there may be large distortions in the raw data that need to be corrected in order to tease out a signal of a systemic effect that needs further attention.
The first of these is mortality displacement. At the end of week 12 in 2021, there had built up about 120,000 excess deaths since the start of the pandemic in the U.K., when compared to the pre-pandemic five-year average.
The median age of these deaths was just under 85 years of age, and it is statistically likely, as mentioned in the Health Foundation report, that around 9% of these deaths would subsequently displace recorded deaths in the following year. This is probably a lower estimate, as it assumes that Covid deaths are in people of average health for their age, which is not generally the case for Covid deaths.
That represents around 10,900 deaths. I therefore amortised this over the period and added it to the non-Covid mortality data.
The second major distortion is due to “deaths due to respiratory diseases as an underlying cause”. According to the ONS, these are about 14% of total deaths.
Much attention has been drawn to the fact that influenza deaths have been largely absent during the past two winters. This is also the case with other respiratory diseases. Whether or not this is a consequence of the Covid virus outcompeting other viruses, or rather some issue like social distancing measures reducing spread, is moot. The important point is they are absent, and this needs to be taken into account as they currently form part of the ‘non-Covid’ deaths in the five-year average and so reduce the estimate of non-Covid excess mortality during the period.
Most of the reductions in excess deaths shown in the Health Foundation report are in line with what you might expect from a 9% mortality displacement. For example, ‘dementia and Alzheimer’s disease’ is down by 11%, stroke 12% and heart disease 4%, all big killers of the segment of the population susceptible to serious Covid. However, ‘influenza and pneumonia’ at minus-48% and chronic lung conditions at minus-25% are way out of sync with that estimate.
The really striking change, however, is the 22% increase in mortality from ‘ill-defined conditions’. Of note also is that there are thousands more deaths recorded by the ONS during the study period with a cardiovascular contribution, whilst deaths with cardiovascular disease as a primary cause are lower (by 4%). Clearly something is badly amiss.
In order to get a true picture of the comparative change from the pre-pandemic five-year average mortality for every cause of death bar Covid and other respiratory diseases, I removed all the mortality data for ‘influenza and pneumonia’ and chronic lung conditions from both the five-year weekly average and the pandemic mortality data.
When both of these actions have been taken, the chart of the non-Covid excess mortality data (below) shows more than 23,000 excess deaths occurring during the study period, which is broadly in line with the number of vaccine injury deaths estimated by Will.
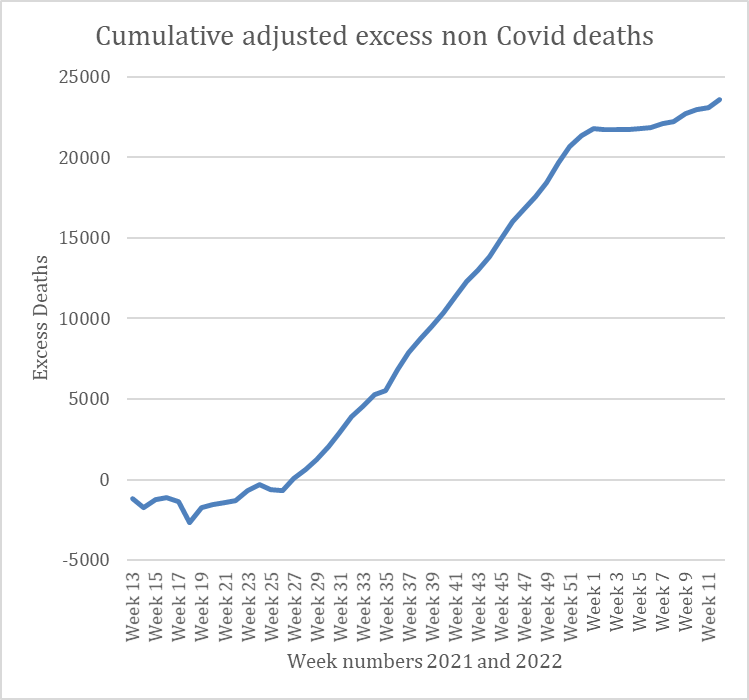
This is a much clearer signal, which has hitherto been hidden in the noise of overall mortality data. It represents causes of death other than Covid or respiratory disease, and indicates that there is a systemic, population-wide effect operating during the study period.
The most likely candidate is the vaccine rollout. The curve shows a steady incline, which is in accordance with the VAERS data for vaccine injury deaths that Will highlighted in his article. The risk versus benefit of these Covid vaccines for large sections of the population will clearly be substantially called into question if the hypothesis is correct.
The rapid and sustained rise in mortality begins around early July. (ER: Vaccine rollout in the UK started in January 2021.) Any prior vaccine deaths may have been masked by the large number of deaths that occurred during the Covid Alpha wave (some of which may have been misattributed to Covid). The sustained increase coincides with the Delta wave and finishes around the time of the Omicron wave becoming prevalent. This may be a coincidence, but alternatively it may warn of a failure of immunity in the population that leaves it vulnerable to major stressors in the environment. The drop in non-Covid deaths during the winter may once again be due to Covid deaths being overcounted and non-Covid deaths undercounted while Omicron was highly prevalent. We see that non-Covid excess deaths have begun rising again in recent weeks.
Is it not time now to halt the vaccination rollout for all those except the most vulnerable in society until this phenomenon is thoroughly investigated? If the hypothesis is correct, each new booster risks further degrading the future health of all who receive them. (ER: Which is therefore a logical defence for not vaccinating anybody!)


••••
The Liberty Beacon Project is now expanding at a near exponential rate, and for this we are grateful and excited! But we must also be practical. For 7 years we have not asked for any donations, and have built this project with our own funds as we grew. We are now experiencing ever increasing growing pains due to the large number of websites and projects we represent. So we have just installed donation buttons on our websites and ask that you consider this when you visit them. Nothing is too small. We thank you for all your support and your considerations … (TLB)
••••
Comment Policy: As a privately owned web site, we reserve the right to remove comments that contain spam, advertising, vulgarity, threats of violence, racism, or personal/abusive attacks on other users. This also applies to trolling, the use of more than one alias, or just intentional mischief. Enforcement of this policy is at the discretion of this websites administrators. Repeat offenders may be blocked or permanently banned without prior warning.
••••
Disclaimer: TLB websites contain copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available to our readers under the provisions of “fair use” in an effort to advance a better understanding of political, health, economic and social issues. The material on this site is distributed without profit to those who have expressed a prior interest in receiving it for research and educational purposes. If you wish to use copyrighted material for purposes other than “fair use” you must request permission from the copyright owner.
••••
Disclaimer: The information and opinions shared are for informational purposes only including, but not limited to, text, graphics, images and other material are not intended as medical advice or instruction. Nothing mentioned is intended to be a substitute for professional medical advice, diagnosis or treatment.