


LOCKDOWN LUNACY 3.0—It’s over.
By J.B. Handley, CHD Contributing Writer
If you’re hoping the COVID-19 pandemic will go on forever, this post may disappoint you. And, I get it. We have gone frothing-at-the-mouth nuts over a slightly above-normal virulence virus, with a unique and obvious age-distribution pattern that should have made containment easy and panic completely unnecessary. And, if you’re living in the United States, like I am, you probably think my declaration that this pandemic is “over” to be somewhere between wishful thinking and incredibly premature, and I hear you, too, although forgive me if I’m not sure you’re the one thinking clearly, given some of the things I’ve recently read. I promise to support my assertion with data, and the wisdom of people far more expert than me who are having a harder time being heard in the present climate of…bats#@t crazy.
Have we lost our collective minds? Yes.
You may not be one of them. In fact, I’m guessing the people who actually take the time to read my blog posts are the few remaining who haven’t been subsumed by the panic, but can we agree that most have? Jeffrey A. Tucker of the American Institute for Economic Research put it best in his excellent essay on July 10 titled, When will the Madness End?:
“I’m a practicing psychiatrist who specializes in anxiety disorders, paranoid delusions, and irrational fear. I’ve been treating this in individuals as a specialist. It’s hard enough to contain these problems in normal times. What’s happening now is a spread of this serious medical condition to the whole population. It can happen with anything but here we see a primal fear of disease turning into mass panic. It seems almost deliberate. It is tragic. Once this starts, it could take years to repair the psychological damage.”
I’m 50 years old, and I’ve noticed that younger people seem particularly scared of COVID-19, they are the ones I typically see biking and hiking with masks on, and this survey really corroborated that point:
The age gradient is striking. The young attach higher probabilities to people like themselves contracting Covid-19, of being hospitalized conditional on infection, and of dying conditional on infection. Arguably, young respondents have a lifestyle that exposes them to wider networks, and this may explain why they feel more likely to be infected. But their assessment of health risks conditional on infection are puzzling in light of the evidence that Covid-19 is significantly less severe for younger people…Third, and crucially, young people, as compared to older people, report substantially higher mortality rates for every age group. Young people are more pessimistic than older people not only about their own mortality risk but also about everyone else’s mortality risk.
Daniel Horowitz wrote a great article about this survey titled, New study: Millennials think their risk from COVID-19 is exponentially more than the true threat. He writes:
Perhaps the most destructive element of lockdown is the panic and fear that such severe measures help confirm, in this case, wrongly so, in the minds of the young and impressionable. As the paper concludes, “Experience has shown that communities faced with epidemics or other adverse events respond best and with the least anxiety when the normal social functioning of the community is least disrupted.” In other words, we need to flatten the fear.
I thought that survey was bad enough, but a different survey by Kekst CNC asking different questions revealed a simply astonishing figure: Americans over-estimated the TOTAL number of compatriots who have died from COVID-19 by 200-fold! When asked the question (in mid-July), “How many people in your country have died from the Coronavirus?”, Americans responded “9%,” which would be roughly 30,000,000 people, versus the actual number of 151,000. No wonder people are panicked (and wildly, wildly misinformed.)
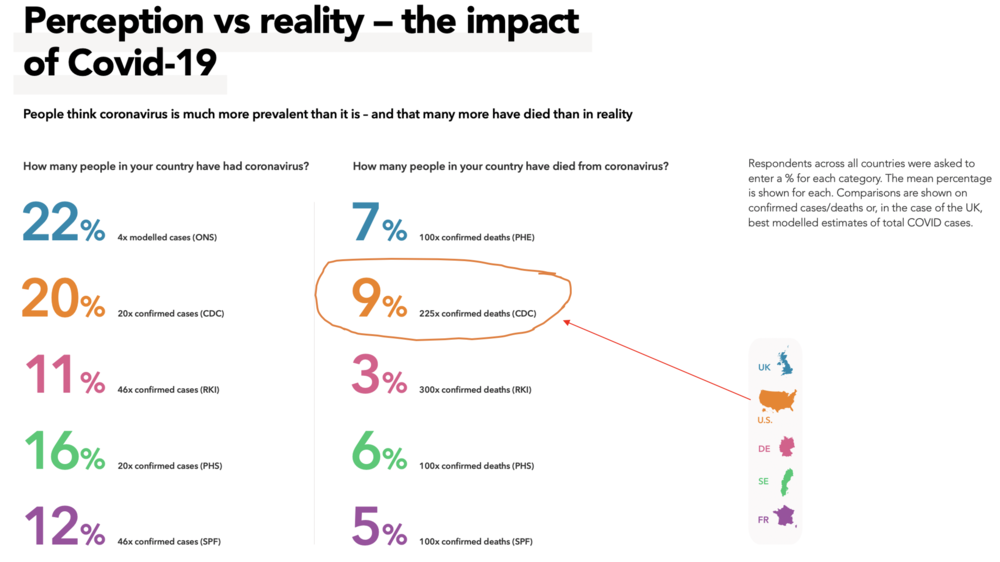
Great, so we can at least agree on three points: 1) Society has lost its collective mind over a virus, and 2) younger people wildly overestimate the risk of dying from COVID-19, which creates a vicious cycle with Point #1, and 3) Americans have wildly overestimated how many people have died from COVID-19.
This is the third time I have written about the pandemic. My first and second blogs provide plenty of data and perspective. I think there are five bits of data that I’ve explored in the past that merit an update:
1. Infection Fatality Rate: The “IFR”, unlike the “Case Fatality Rate” that is more often quoted in the news, is the ACTUAL fatality rate of COVID-19. In order to accurately forecast the IFR, you need two bits of data: total deaths, and total people who have had the virus. The second data point is harder to find, because so many people are asymptomatic, but the most reliable data I have found is in this meta-analysis by Stanford’s Dr. John Ioannidis titled, The infection fatality rate of COVID-19 inferred from seroprevalence data. What does the paper conclude? A median IFR of 0.25%. It’s hard to make this point strongly enough: a virus with an IFR this low would never, ever merit the response we’ve seen from health authorities and elected officials. COVID-19 is hardly a “once in a century pandemic” as some try to say, it’s a strong flu bug, nothing more.
2. Death rates by age stratification. The best science I have seen showing IFR by age is this study titled Assesssing the Age Specificity of Infection Fatality Rates for COVID-19: Meta-Analysis & Public Policy Implications. Check out this chart:
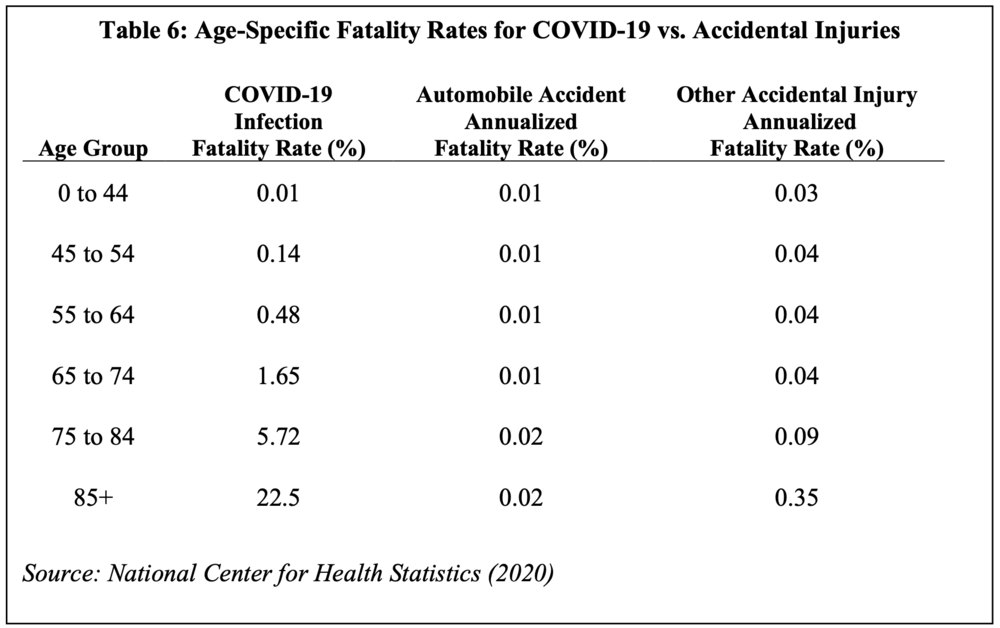
I wish this chart broke the age down even further, particularly in the 0-10 or 0-20 age range, where the IFR is effectively zero. These facts are slowly making their way into the mainstream, and the paper concludes: “Age and fatality risk for COVID-19 are exponentially related. In non-technical terms, COVID-19 poses a very low risk for children and younger adults but is hazardous for middle-aged adults and extremely dangerous for elderly people.”
3. Herd Immunity Threshold. Since my previous blog post, when I wrote about Herd Immunity Threshold in detail, it’s becoming even more clear that the “H.I.T.” of COVID-19 is very likely in the 10-20% range, rather than the 60-70% range that was originally thought. It would be impossible to overstate the importance of this difference, because it supports exactly WHY COVID-19 has already reached herd immunity in most of Europe, and WHY we’re almost done here in the U.S., too. Here’s one new paper, Herd immunity thresholds for SARS-CoV-2 estimated from unfolding epidemics. Their conclusion:
Our inferences result in herd immunity thresholds around 10-20%…these findings have profound consequences for the governance of the current pandemic given that some populations may be close to achieving herd immunity despite being under more or less strict social distancing measures.

The conclusion that COVID-19’s H.I.T. is between 10-20% is gaining wide acceptance, and it’s being borne out in the real world as countries everywhere are watching deaths from COVID-19 simply dry up, as the virus runs out of new people to infect. The obvious explanation for WHY the H.I.T. for COVID-19 is far lower than thought is that many more of us are naturally immune to COVID-19, because our T-cells carry immunity based on the fact that we’ve all been exposed to many corona viruses, which is commonly called a cold. My favorite outspoken scientist on this issue is Oxford’s Dr. Sunetra Gupta, check out this interview with her titled, “We may already have herd immunity – an interview with Professor Sunetra Gupta.” A quote:
What I didn’t anticipate was that some of our responses to previous exposure to seasonal coronaviruses might actually protect us from infection. It’s one thing to get infected and not ill, but what the new studies are showing is that people are actually fighting off infection. So at an even more basic level, the pre-existing antibodies or T-cell responses against coronaviruses seem to protect against infection, not just the outcome of infection.
If you read one link in this whole blog post, I’d make it this interview with Dr. Gupta, it’s wide-ranging and she also explains how lockdowns not only don’t work (see next) but that countries and states that sealed themselves off—like New Zealand or Hawaii—are simply postponing their day of reckoning. Dr. Gupta and her team’s new paper, The impact of host resistance on cumulative mortality and the threshold of herd immunity for SARS-CoV-2, explores the issue of H.I.T. further:
These results help to explain the large degree of regional variation observed in seroprevalence and cumulative deaths and suggest that sufficient herd-immunity may already be in place to substantially mitigate a potential second wave.…Equally, seropositivity measures of 10-20% are entirely compatible with local levels of immunity having approached or even exceeded the HIT, in which case the risk and scale of resurgence is lower than currently perceived.
4. Lockdowns don’t work. Getting politicians involved in trying to fight the normal course of a viral illness will hopefully be seen my historians as one of the silliest things we ever chose to do. In simple terms, a virus is gonna be a virus. As Dr. Gupta explains, “The epidemic is an ecological relationship that we have to manage between ourselves and the virus. But instead, people are looking at it as a completely external thing.” Said differently, like every other virus, COVID-19 is here to stay. Lockdowns provide politicians with an “illusion of control” but the data is rolling in that they have been useless, and even The Lancet, one of the world’s most prestigious medical journals, has weighed in. Titled, A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on COVID-19 mortality and related health outcomes, their conclusions are pretty stark, and depressing for those of us who have undergone lockdowns:
“Government actions such as border closures, full lockdowns, and a high rate of COVID-19 testing were not associated with statistically significant reductions in the number of critical cases or overall mortality.”
German scientists looked at the same topic just within the country of Germany and reached the same conclusion in this paper titled, Change points in the spread of COVID-19 question the effectiveness of nonpharmaceutical interventions in Germany. An excerpt:
A trend change of infections from exponential growth to decay was not induced by the “lockdown” measures but occurred earlier. Additional impacts of later NPIs cannot be clearly detected: Firstly, there is no significant effect with respect to infections that could be attributed to school and day-care closures. Secondly, effects which could be related to the contact ban a) do not appear with respect to all three indicators, b) differ in strength and tend towards lower impacts, and c) do not match the time the measure came into force. Thus, the necessity of the second (March 16-18) and the third bundle of interventions (March 23) is questionable…
All these American Governors threatening to resume lockdowns? Yes, there’s no science that supports anything they are threatening. A virus is going to be a virus, which leads me to the final piece of data before we look at the evidence that inspired the title of this piece, the evidence that the pandemic is OVER.
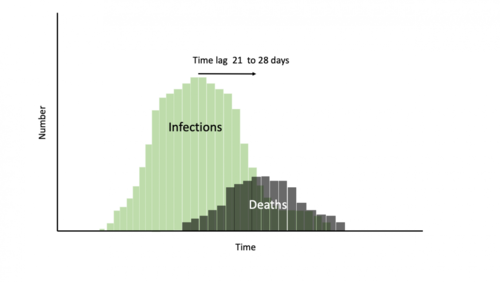
5. Viruses go up, and then down, and the death rate is the only reliable way to track them. A team at Oxford explains this way better than I ever can. In this post titled COVID-19: William Farr’s way out of the Pandemic, they explain how Farr, a UK epidemiologist from the mid-19th century, understood that all viruses follow a similar pattern, and that the slope of the death curve on the way up will roughly equal the slope on the way down, which means if you know when you have reached peak deaths, you have a very good idea of when the virus will be extinguished. As Farr wrote, “The death rate is a fact; anything beyond this is an inference.” The Oxford scientists write:
Once peak deaths have been reached we should be working on the assumption that the infection has already started falling in the same progressive steps. Using deaths as the proxy for falling infections facilitates the planning of the next steps for reopening those societies that are in lockdown.
I think there are two points about Farr’s Law that deserve further clarification: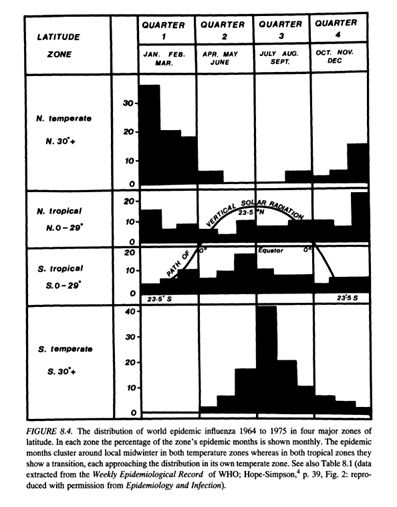
- In order to prove the virus is basically done, I’m going to be showing you death curves from all over the world. My death curves are based on country-specific reported COVID-19 deaths. This runs the risk that COVID-19 deaths are overstated because of the pressure in many places to classify any questionable death as a COVID-19 death. The proper way to measure the impact of a virus is to compare current year “all cause mortality” versus previous year “all cause mortality.” This is a far more accurate way to see IF COVID-19 impacted mortality, and the way Farr recommended doing it.
-
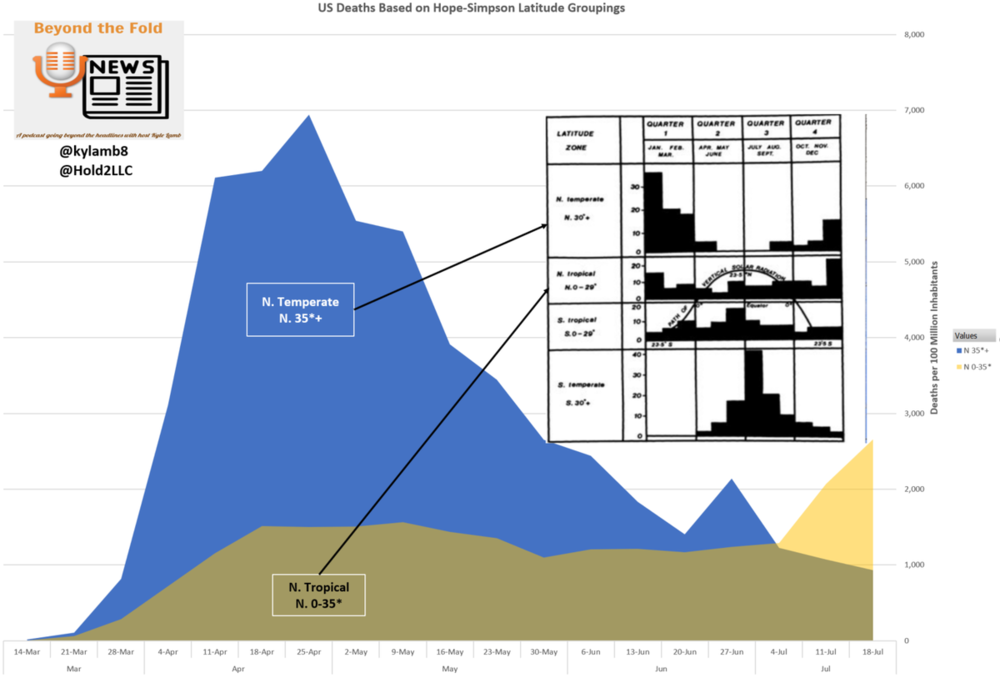
I missed something when I wrote my previous blog post. While Farr has been proven right, that viruses typically have the same death slope on the way up and down, I missed the wisdom of another British scientist, Dr. Edgar Hope Simpson, who explained that the course of a virus is DIFFERENT in terms of both timing and its slope, based on WHERE in the world you live, by latitude. Whether driven by solar radiation or Vitamin D levels, Hope-Simpson long ago predicted exactly what happened in California, Arizona, Texas, and Florida in the last month: COVID-19 came later, on a lower death curve, to U.S. states that sit at or below the 35th parallel (see chart from his book that shows this visually). Hope-Simpson’s seminal work is a book titled The Transmission of Epidemic Influenza, and why our public health authorities never discuss the fact that seasonal viruses hit our lower latitudes later in the year is beyond me. The U.S. is unique, relative to Western Europe, because our geography is so vast. In simple terms, our northern states are done with their death curves, and our southern states are almost there. Read on.
It’s over when the death curve says it’s over
Now we get to the fun part: celebrating that the COVID-19 pandemic is over in most Northern countries and passed the peak in most Southern countries. In the United States, we actually have two distinct death curves, roughly divided along the 35th parallel. The Northern states are done, and the Southern states are almost done. I’ll start with the rest of the world, and finish with the U.S. Please note that ALL the death curve charts I’m using come from Worldometers, so you can go see the exact same ones for yourself. Are they imperfect? Yes. But, they are the best we have. Will I give you an actual date for the U.S.? Yes, I will.
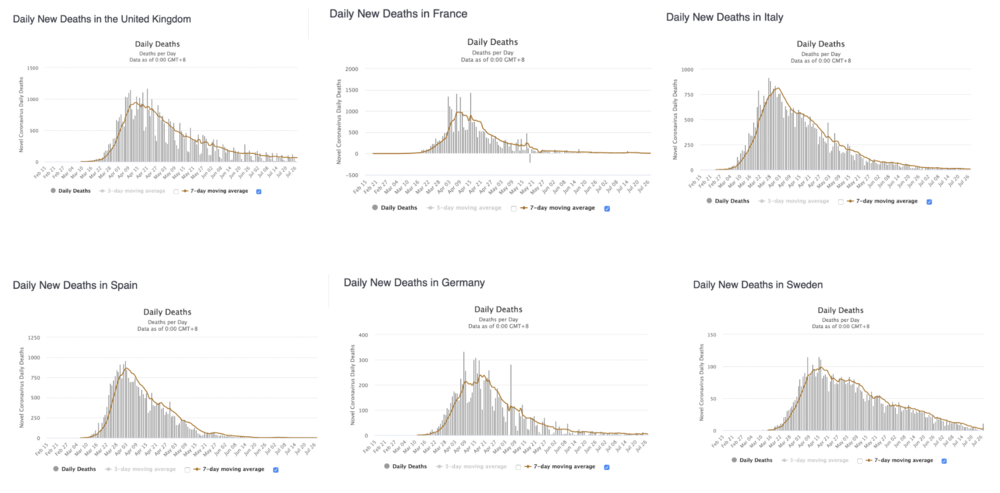
Europe
Here are the death curves, from Worldometers, for six European countries. It’s self-explanatory, so I won’t belabor the point. To state the obvious: Sweden had no lockdown. Amongst the other five countries, the choice for HOW to lockdown varied widely. Knowing those simple facts and seeing these charts, if you still think lockdowns are important in the management of a seasonal virus, I can’t help you. In Western Europe, IT’S OVER, and it had nothing to do with how governments, or the populace, behaved. A virus does what a virus does.
U.S. Northern States
Using the same data from Worldometers, it’s also over in the northern states. Note that in certain states, the impact from COVID-19 is so tiny, the death curves aren’t even curves, so I’m focusing on larger population states that actually have a curve. I looked at New York, New Jersey, Massachusetts, Illinois, Indiana, and Michigan.
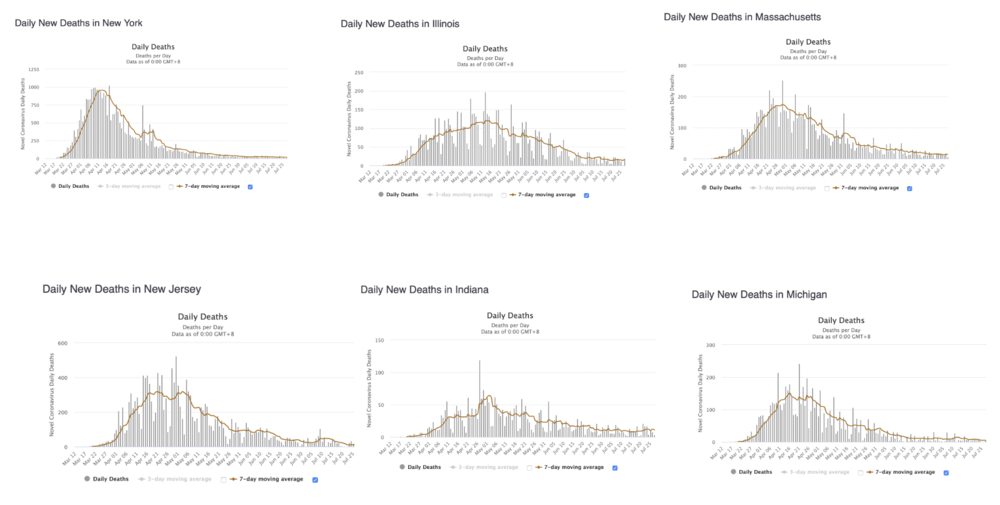
In the Northern U.S states, IT’S OVER, and it had nothing to do with how governments, or the populace, behaved. A virus does what a virus does.
U.S. Southern States
This quote from Dr. Gupta of Oxford explains the mistake the press keeps making by treating the U.S. so homogeneously:
When you think of the US as a whole, you’re missing the fact that the epidemic appears to be over in the north east and growing in the south west. Why would you put them together? There’s no reason to lump a rise in cases in Arizona with everything else.
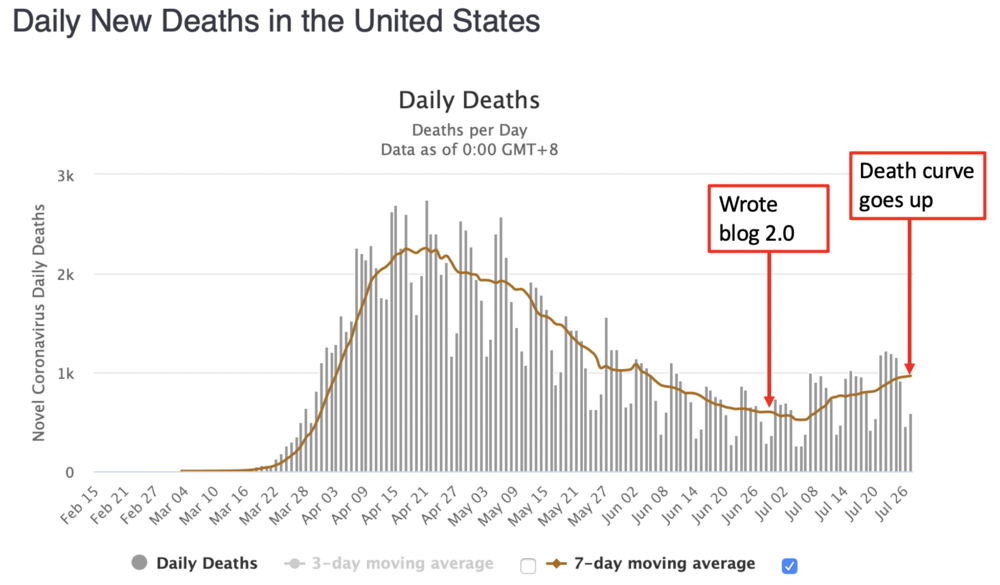
This is the most confusing part of predicting when the COVID-19 pandemic will be over in the United States. Take a look at the TOTAL U.S. death curve when I wrote my last blog post, and where it is today:
What happened? Seasonal viral patterns of southern latitude states. Well, luckily for me, some smart and enterprising analysts graphed the U.S. death curve, but did something different, they separated the states by using the division of the 35th parallel, basically turning us into two separate countries. They had to make some judgments, so ALL of California is in the Southern number, and here’s how the death curves looks:
This is an excellent quick video that explains this seasonal dynamic:
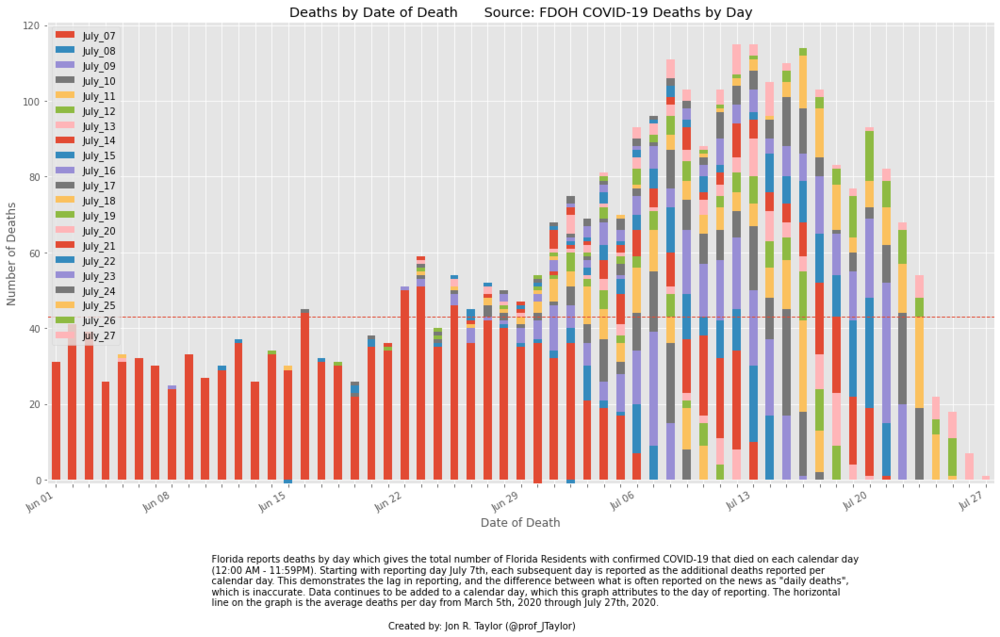
There’s plenty of data showing that the southern states are all past their peak. Here’s deaths in Florida, sorted by date of death, the curve is clear:
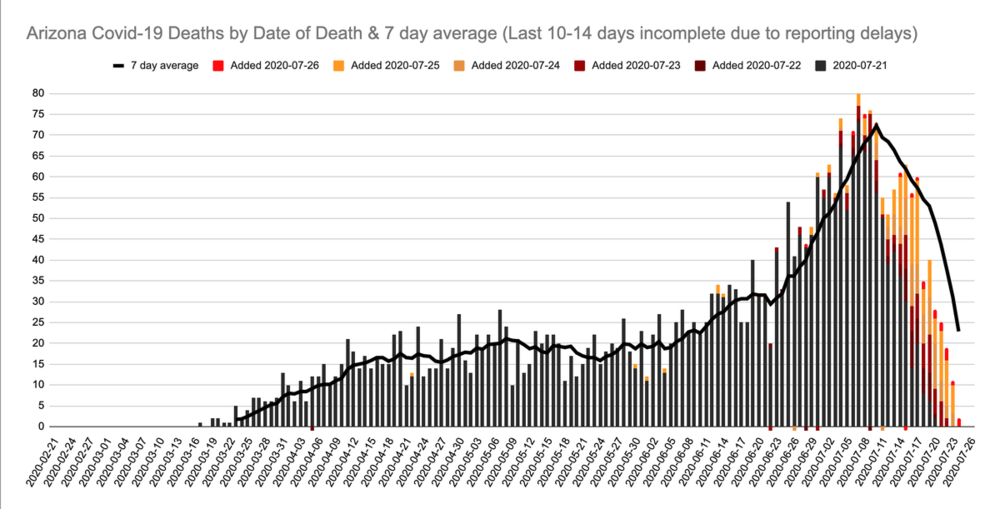
Here’s deaths in Arizona:
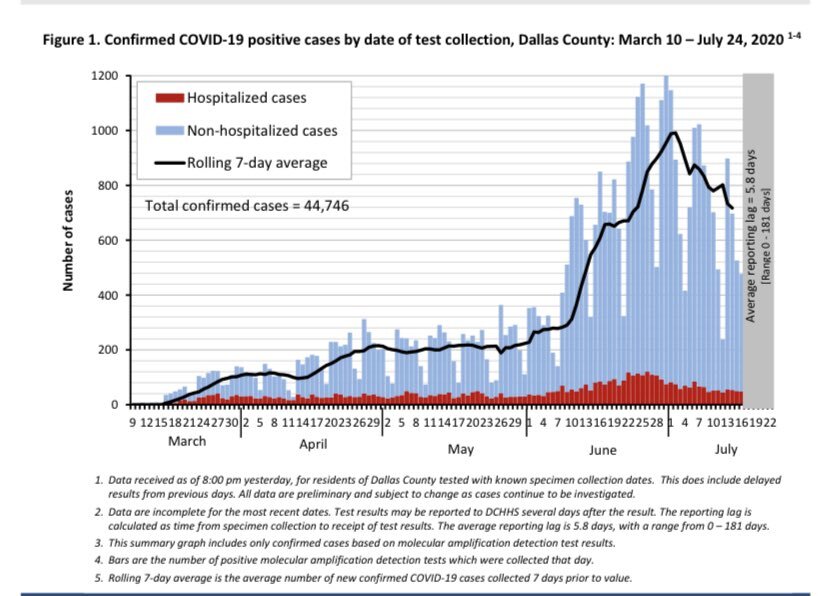
And here’s the hospitalization curve in Texas, showing well past peak, death curves always match hospitalization curves with a minor lag.
So when will it be over in the United States?
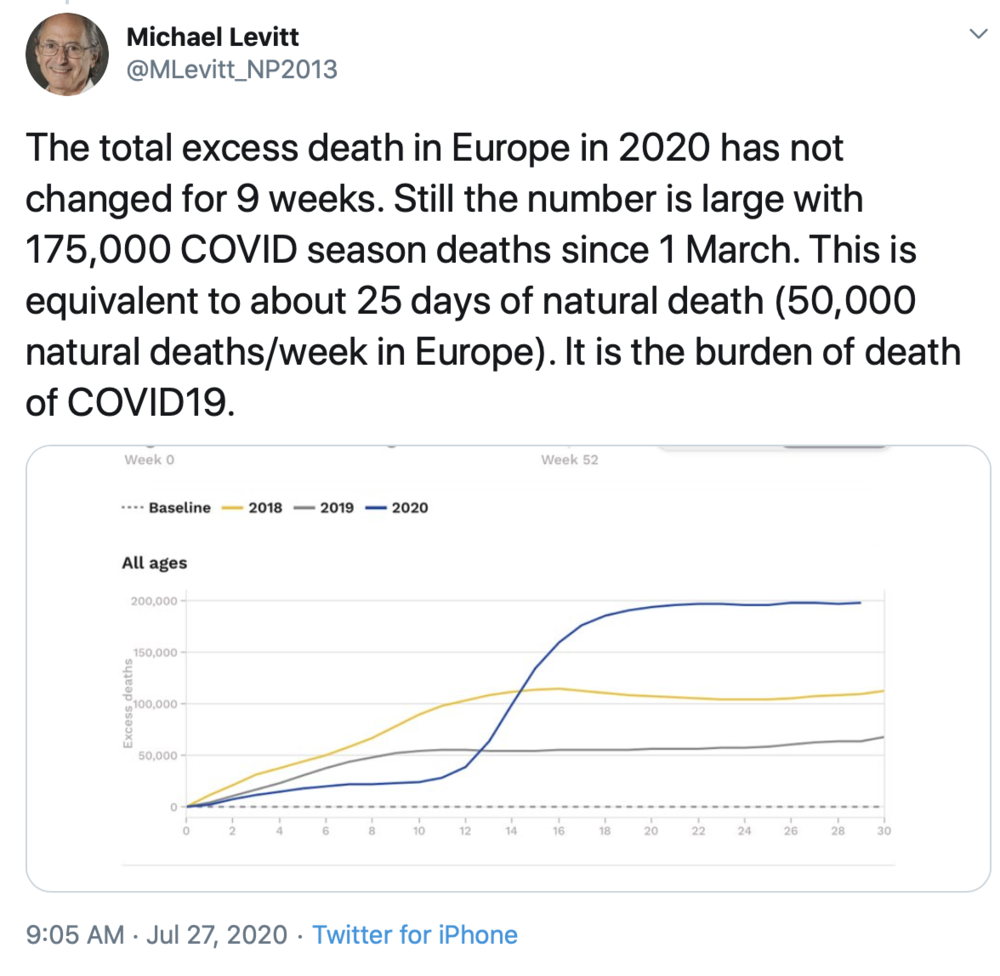
That’s the question you’ve patiently been waiting for me to answer. When will we be done in the United States? August 25th, just under one month from now. How do I know that? Well, I don’t know it with certainty, but it’s the date that Stanford Nobel laureate Dr. Michael Levitt picked and he’s been right on China and Sweden, so I’m going with him. Let’s explore his answer to this question and how he looks at it.
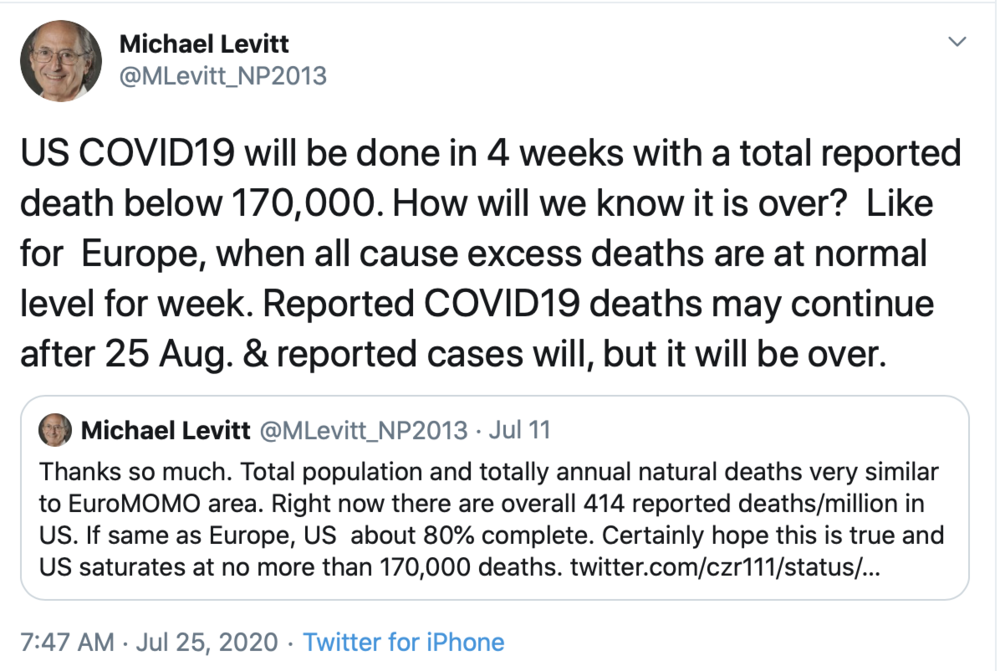
Dr. Levitt does exactly what William Farr said to do: he looks at historical all-cause mortality, and when we hit that same threshold here in the U.S., the pandemic is over. His analysis shows we get there by August 25th. He explains why Europe is already done, the excess deaths from COVID-19 have stopped now for several weeks, which is what all the death curves I showed you above also corroborate.
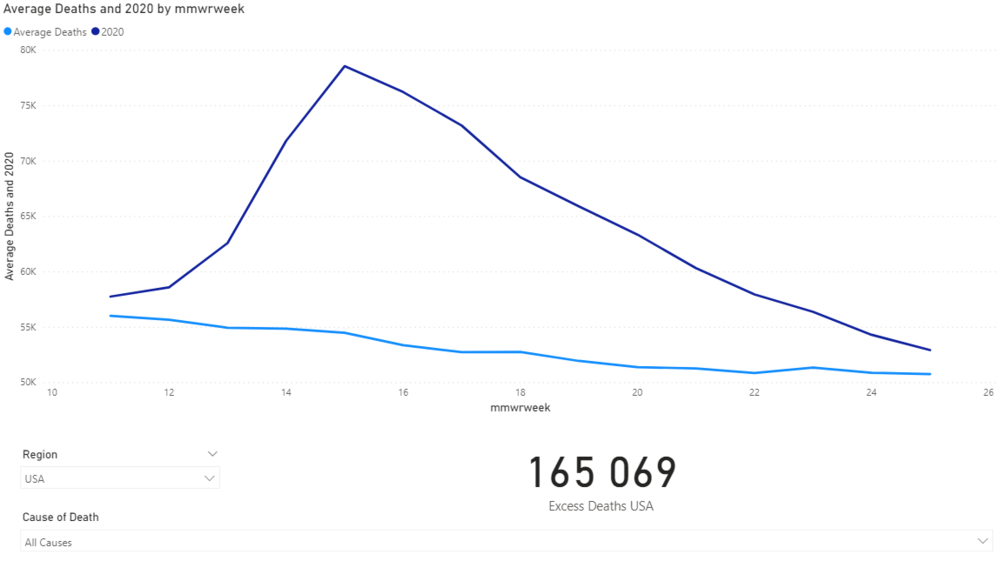
Interestingly looking at CDC data, the 2020 death curve and the Average Death Curve in the U.S. are extremely close to converging, we may be done even sooner than we think:
Conclusion
It’s over in most of the world. It will likely be over in the United States within the next four weeks. You can spend your time watching the news and hearing about “new cases” and being worried, or you can get on with your life, I’m opting for the latter. I’ll finish with a great quote from Oxford’s Dr. Gupta that summarizes how I feel about this whole mess:
The truth is that herd immunity is a way of preventing vulnerable people from dying. It is achieved at the expense of some people dying, and we can stop that by preventing the vulnerable class in the process. In an ideal situation, you would protect the vulnerable as best you can, let people go about their business, allow herd immunity to build up, make sure the economy doesn’t crash, make sure the arts are preserved, and make sure qualities of kindness and tolerance remain in place.
Appendix
Since I last wrote, there have been a few articles that really jumped out to me. Here’s a few great ones:
Wired Magazine, It’s Ridiculous to Treat Schools Like Covid Hot Zones
Excerpt:
Let’s review some facts: Children are, by and large, spared the effects of the virus. According to the latest data from the CDC, infants, little kids, and teenagers together have accounted for roughly 5 percent of all confirmed cases, and 0.06 percent of all reported deaths. The Covid-linked child inflammatory syndrome that received fervent media attention last month, while scary, has even more infinitesimal numbers. “Many serious childhood diseases are worse, both in possible outcomes and prevalence,” said Charles Schleien, chair of pediatrics at Northwell Health in New York. Russell Viner, president of the UK’s Royal College of Pediatrics and Child Health, noted that the syndrome was not “relevant” to any discussion related to schools.
There is also a wealth of evidence that children do not transmit the virus at the same rate as adults. While experts note that the precise transmission dynamics between children, or between children and adults, are “not well understood”—and indeed, some argue that the best evidence on this question is that “we do not have enough evidence”—many tend to think that the risk of contagion is diminished. Jonas F. Ludvigsson, a pediatrician and a professor of clinical epidemiology at Sweden’s Karolinska Institute, reviewed the relevant research literature as of May 11 and concluded that, while it’s “highly likely” children can transmit the virus causing Covid-19, they “seldom cause outbreaks.” The World Health Organization’s chief scientist, Soumya Swaminathan, suggested last month that “it does seem from what we know now that children are less capable of spreading” the disease, and Kristine Macartney, director of Australia’s National Centre for Immunisation Research and Surveillance, noted a lack of evidence that school-aged children are superspreaders in her country. A study in Ireland found “no evidence of secondary transmission of Covid-19 from children attending school.” And Kári Stefánsson, a leading researcher in Iceland, told The New Yorker that out of some 56,000 residents who have been tested, “there are only two examples where a child infected a parent. But there are lots of examples where parents infected children.” Similar conclusions were drawn in a study of families in the Netherlands.
The Atlantic, Hygiene Theater Is a Huge Waste of Time
Excerpt:
COVID-19 is apparently a war that will be won through antimicrobial blasting, to ensure that pathogens are banished from every square inch of America’s surface area.
But what if this is all just a huge waste of time?
In May, the Centers for Disease Control and Prevention updated its guidelines to clarify that while COVID-19 spreads easily among speakers and sneezers in close encounters, touching a surface “isn’t thought to be the main way the virus spreads.” Other scientists have reached a more forceful conclusion. “Surface transmission of COVID-19 is not justified at all by the science,” Emanuel Goldman, a microbiology professor at Rutgers New Jersey Medical School, told me. He also emphasized the primacy of airborne person-to-person transmission.
Paul Graham, The Four Quadrants of Conformism
Excerpt:
One of the most revealing ways to classify people is by the degree and aggressiveness of their conformism. Imagine a Cartesian coordinate system whose horizontal axis runs from conventional-minded on the left to independent-minded on the right, and whose vertical axis runs from passive at the bottom to aggressive at the top. The resulting four quadrants define four types of people. Starting in the upper left and going counter-clockwise: aggressively conventional-minded, passively conventional-minded, passively independent-minded, and aggressively independent-minded.
I think that you’ll find all four types in most societies, and that which quadrant people fall into depends more on their own personality than the beliefs prevalent in their society. [1]
Spiegel International, Reconstruction of a Mass Hysteria
Excerpt:
The new virus would probably have attracted far less attention if it hadn’t been for modern molecular medicine, with its genetic analyses, antibody tests and reference laboratories. The swine flu would have conquered the world, and no doctor would have noticed.
But the world did notice, largely because of high-tech medicine and the vaccine industry. From Ebola to SARS to the avian flu, epidemiologists, the media, doctors and the pharmaceutical lobby have systematically attuned the world to grim catastrophic scenarios and the dangers of new, menacing infectious diseases.
None of these diseases receives more attention than influenza. Researchers in more than 130 laboratories in 102 countries are constantly on the lookout for new flu pathogens. Entire careers and institutions, and a lot of money, depend on the outcomes of their work. “Sometimes you get the feeling that there is a whole industry almost waiting for a pandemic to occur,” says flu expert Tom Jefferson, from an international health nonprofit called the Cochrane Collaboration. “And all it took was one of these influenza viruses to mutate to start the machine grinding.”
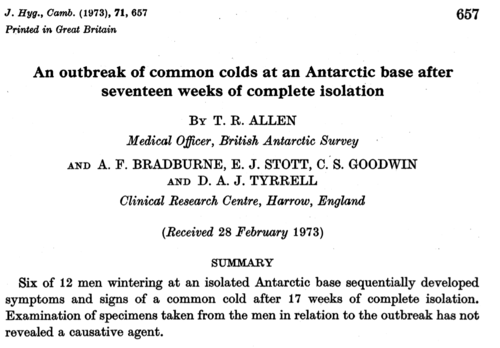
T.R. Allen, An outbreak of common colds at an Antarctic base after seventeen weeks of complete isolation
 Comment:
Comment:
This is a published study from 1973, and the title kind of gives it away, but basically six of seventeen men wintering at a base in Antarctica got sick with a cold (coronavirus) “after 17 weeks of complete isolation.” If you weren’t sure if a virus is going to do what it’s going to do, I hope this gives you pause. (Are you listening, New Zealand?) Part of their conclusion is quite the omen for today’s craziness: “The occurrence of a common cold during isolation, when the chances of introduction of new infection from the outside are virtually nil, implies that in some way virus persisted, either in the environment or in the men.” Look out.
About the author: J.B. Handley is the best-selling author of How to End the Autism Epidemic. He graduated with honors from Stanford University, and currently serves as a Managing member of Bochi Investments, a private investment firm. He can be reached at [email protected]
••••
The above article LOCKDOWN LUNACY 3.0—It’s over originated on Children’s Health Defense and is re-published here by contribution with attribution to the author J.B. Handley and Children’s Health Defense.
••••
TLB Editors Note: This is World Mercury Project on steroids! TLB highly recommends you click on the image below, visit this great website, and do whatever you can to help see this vital forum succeed … for the sake of our children !!!
Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. CHD is planning many strategies, including legal, in an effort to defend the health of our children and obtain justice for those already injured. Your support is essential to CHD’s successful mission.

••••

••••
Stay tuned to …

••••
The Liberty Beacon Project is now expanding at a near exponential rate, and for this we are grateful and excited! But we must also be practical. For 7 years we have not asked for any donations, and have built this project with our own funds as we grew. We are now experiencing ever increasing growing pains due to the large number of websites and projects we represent. So we have just installed donation buttons on our websites and ask that you consider this when you visit them. Nothing is too small. We thank you for all your support and your considerations … (TLB)
••••
Comment Policy: As a privately owned web site, we reserve the right to remove comments that contain spam, advertising, vulgarity, threats of violence, racism, or personal/abusive attacks on other users. This also applies to trolling, the use of more than one alias, or just intentional mischief. Enforcement of this policy is at the discretion of this websites administrators. Repeat offenders may be blocked or permanently banned without prior warning.
••••
Disclaimer: TLB websites contain copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available to our readers under the provisions of “fair use” in an effort to advance a better understanding of political, health, economic and social issues. The material on this site is distributed without profit to those who have expressed a prior interest in receiving it for research and educational purposes. If you wish to use copyrighted material for purposes other than “fair use” you must request permission from the copyright owner.
••••
Disclaimer: The information and opinions shared are for informational purposes only including, but not limited to, text, graphics, images and other material are not intended as medical advice or instruction. Nothing mentioned is intended to be a substitute for professional medical advice, diagnosis or treatment.

Thank you very much for this article. Just yesterday I was politely asked either to wear a mask or to leave the store, a store which specializes in leather-making tools and goods in Cheyenne, Wyoming. I opted for leaving the store. Still, I want to follow up that experience with a letter to the store manager and also to the company’s headquarters in Fort Worth, Texas, and I’m hoping that a reference to this article, or perhaps a reference to it _and_ a hard copy of it, might help alleviate some of the fear gripping so many of today’s decision-makers, assuming fear is what’s driving draconian decisions. Thanks again. I plan to put your research to good use.
Thank you so much Mr Handley – excellent article. This should be sent to every member of the general public and they should be forced to read it.
!!! GOOD-BYE AMERICA, AND WELCOME TO THE FOURTH REICH !!!—:::
https://www.nowtheendbegins.com/cdc-covid-19-coronavirus-vaccine-joint-venture-dod-pentagon-department-defense/