


ER Editor: This detailed, insightful reporting may give us glimmers of hope that dawn is finally breaking in the minds of medical personnel about the harmful effects of the Covid vaccines.
However, what it clearly and convincingly shows is how FRAUD was SYSTEMATICALLY PERPETRATED ON MEDICAL STAFF by ‘The System’, and how many of them fell for it hook, line and sinker. How? By having sick-through-Covid-vaccination patients show up in hospitals where medical staff were led to believe that they were UNvaccinated. Thus, they were more likely to take up the vaccine themselves. And were more likely to disparage the unvaccinated.
While this report focuses on the US medical system, we’ve heard similar echoes in the UK’s NHS ‘system’ (a word we now loathe) as well as others.
********
Nursing Reports From The Front Lines Of The COVID Vaccine Crisis
The massive propaganda campaign which led doctors to disassociate from the reality of widespread vaccine injuries is slowly weakening in impact. A stark reality is finally creeping in.

I recently posted a deeply referenced compilation of evidence detailing the historic humanitarian catastrophe that has slowly unfolded within most advanced health economies across the world. Caused by a global mass vaccination campaign led by the Pharma masters of BMGF/WHO/CDC that illogically (but profitably) targeted a rapidly mutating coronavirus. They did it with what turned out to be the most toxic protein used therapeutically in the history of medicine. In vials mixed with lipid nano-particles, polyethylene glycol and who knows what else.
I cited studies and reports showing massive increases in cardiovascular deaths and neurologic (and other) disabilities amongst working age adults, beginning in 2021 only. A disturbing signal screaming from the original clinical trials data, VAERS data, life insurance data, disability data, reports of cardiac arrests of professional athletes, rises in ambulance calls for cardiac arrests in pre-heart attack age young people, and the massive increases in illnesses and data manipulations in Department of Defense databases.
As these events become more and more recognized by the average citizen (and occasional journalist), a new pathetic “Disinformation Campaign” was launched in response trying to blame all the young people dying as simply a need for increased awareness of the rare condition called Sudden Adult Death Syndrome (SADS), rather than examples of the legions dying from the vaccines. The fact checkers also came out in support of this narrative, branding anyone who thinks the vaccines are the cause of SADS as a conspiracy theorist. Like this self-appointed social media watchdog. Mentions of SADS are popping up from many countries.. all in the last few weeks. Here, here, here, here and.. oh whatever. This article even listed a dozen such publicized deaths in the past few weeks from all over the world..but blamed them all on SADS. You get it. What is nauseating is the tone of purported good intentions within these articles, informing folks that if you are related to someone young who died suddenly, you should go see a cardiologist to make sure you don’t have an abnormal EKG. After it turns out normal, they will assuredly tell you to get vaccinated, an absurdity atop a mountain of absurdities caused by our bio-medical-media industrial complex over the past 2+ years.
Ugh, let’s move on. In this post, I will move away from numbers and data and studies to give a more qualitative view of how the vaccines’ impacts are manifesting in the “belly of the beast,” (i.e. on the inside of a major academic medical center).
I want to first share a comment made in response to another recent post of mine, by my new partner in our COVID/Long Haul/Vax Injury specialty tele-health practice. Scott Marsland is both a COVID-expert and a Nurse Practitioner Extraordinaire (you should see the reviews he gets by his patients – they are over-the-top). Anyway, Scott wrote:
The most profound reflection of this last week came from a patient who is a physician and therapist. She was hospitalized recently for non-COVID reasons and observed: “I think many of the physicians are exhibiting dissociation. It takes an enormous amount of energy to maintain their narrative and hold off the reality hitting them in the face every day.” I thought of this reading the recent piece you referenced from The Annals of Emergency Medicine.
Wikipedia:“The major characteristic of all dissociative phenomena involves a detachment from reality, rather than a loss of reality as in psychosis. Research has suggested that dissociation is inversely related to mindfulness, which is a potential treatment.“
TY PK for this dose of mindfulness.
I thought his comment was the perfect introduction to this post, where I will share disturbing “insider info,” compiled largely from recent correspondences with a senior ICU and ER Nurse, both via email and phone. Although she is not working full-time in ICU’s or ER’s anymore, she still does shifts on occasion, particularly night shifts. Night shifts, although brutal, are WAY more fun and relaxed than day shifts. That is, most of the time, unless you get slammed due to less staff being around. Although the worst shifts of my career were night ones, thankfully they were rare.
What is great about night shifts is the camaraderie and closeness that develops among staff that choose to primarily work nights. The pool of such folks is small, and they choose night shifts for various but often similar reasons (preference, child care responsibilities, other jobs, hatred of day shifts etc). The general atmosphere is more “intimate,” as you end up having conversations, longer and deeper than you would or could in the middle of a hospital day. This is because at night there are no families around, no administrators, most patients are sleeping (sort of), no masses of swirling ancillary specialists like dietitians, physical therapists, occupational therapists, speech therapists, physician sub-specialists, transporters, social workers, food service workers, maintenance folks etc.
Anyway, this was the first email I received from her (editorial note: I wrote out or translated all her abbreviations but made no other edits to substance – I had to do it as her writing style clearly reflected someone who has been writing myriad nursing notes her whole career :).
On May 12, 2022, at 7:47 PM, L. <XXXX> wrote:
I wish I could have you as my doc. Nurse of 20 yrs + ICU – cardiac, neuroICU/ neurosurgical ICU mostly, and ED at Level 1. Vax injured from 2 Pfizer doses mandated by my major University hospital system. Clotting issues, open bleeding, spontaneous with no ability to stop, weeping down arms and legs. Severe leg clot post-surgery in March. Had to get D-Dimer ordered by force at little ED I was in, and use my own portable doppler I brought in from work, b/c they had no Ultrasound techs or equipment access – TPA (clot buster med) finally. Cervical lymph nodes enlarged since vax especially, for over 1.5 yrs. Cannot biopsy at least one as it sits on my Left carotid, now wrapped around it, . Got Covid originally while working ED in March 2020. “N antibody” still high as of Nov 2021. Hit neuro, never respiratory. Had same issues with H1N1 vaccine which was also mandated and then I got Guillain Barre Syndrome and neurological weakness – out of work 5 months. Will not get any boosters or vaccines this year, but have no exemption as all docs took to the “deer in headlight” look and said nothing. I will lose my career this winter if I refuse. Functional med/family practitioner – she has a long wait list and I have no idea how she sits with this data on vaccine injured. My VAERS report – it was deleted. Pharmacist never entered as required so I did. It has vanished. My batch numbers – significant for bad neurologic responses, clotting. I lost my Hematologist-Oncologist doctor to vaccine injury – he is out and never to practice again – in his early 40s. He was a “true believer” and in denial until it was him who was the injured patient. Our cancer hospital – know most of the case managers and many doctors since they were residents. They now have case loads in the 1000s rather than 250-400 over any given quarter. Not enough bed or infusion space for the cancer patients as outpatients. Radiation treatment backlog. All at a huge cancer hospital monstrosity itself. All kinds – brain, lymph, stomach, pancreas, blood, AND EYE CANCERS – orbital especially in younger people recently vaxxed. Microvascular ischemia on rise in vaxxed younger people. Strokes way up in no-risk, no co-morbidities, young to younger-ish. Ask me anything. I’ll tell you inside scoop from the floors and suites. This has to stop. They need to admit the fraud and crime and STOP. The liability must be lifted, mandates ended. They KNOW NOW and many KNEW THEN. Don’t know if you’ll even read this, but I follow all of you on substack and Twitter – those not banned yet! – and read ALL the data. I’ve been a lab rat myself from an issue from a car accident yrs back – I know the process. So much fraud. Keep going. Never give up. Never, never, never give up. Thank you for all you do, hope that you inspire and the confirmation of that little voice in me, that said NO way back, everything was off. I did not have an option or data then. I have data now, and it will keep coming. The option is NO.
Follow up:
Lost 4 practitioners to serious side effects of “strongly encouraged” boosters. 2 hospitalized, one in MICU. The irony is, for most staff, completely lost ….All in early 30s to mid 40s. They had no need for boosters while BEING OUTSIDE ALL WEEKEND even if they truly believed in efficacy of them. All had Covid previous, N antibodies fully measurable. One female, one male, both inpatient. Female still nursing newborn.
On Fri, May 13, 2022 at 11:27 AM Pierre Kory <> wrote:
I am stunned by your email. Stunned. We know it’s bad, like real bad but this is the worst inside look I have heard yet. I am on the outside and don’t talk to most former colleagues so don’t have a feel. We should talk. Would you be interviewed on a VSRF (Kirsch’s organization) webinar? I assume not, but who knows, maybe anonymously like with altered voice and blurry screen? This needs to get out. Send me contact.. and name? First name is fine.. Thanks for this – Pierre
She wrote again before we talked, it was this email below that prompted me to ask her number so we could discuss in more depth:
It’s the inside folks who talk to each other, and you have to speak another language depending on who’s listening. That has been a skill set unto itself. It’s texting, the phone calls from area to area with back stories on patient issues. I was getting texts from my old stat team covering cardiac catheterization lab – the clots. The clots stunned everyone…it continues. My cardiac units – where I spent the bulk of my nursing years – lung and heart transplant included – have so many anomalies presented with patients that never existed before. Re-writing the script for each new problem never encountered. The constant codes (cardiac arrests). Can’t keep up.
Lost quite a few coworkers to either VAX injury itself – took them out of the work force, OR they resigned/accepted firing or retired once mandates were settled. It’s the phone calls I have with my cohorts in the other areas of the system. The real story is in those conversations. The doctors now admitting to injury is growing, but they can’t tell their patients why they are no longer practicing. Losing specialists is big problem not easily solved.
The signaling coming from management MD/PhD administrators has not been towards what winter will bring, but is focused on congratulating everyone on clinical excellence during the last 2 yrs. I think there is great trepidation in their approach because they see the data, they know the inside info on injury, disability/death of faculty and staff not from Covid itself, but the forced vax. We lost only a few to original Covid, with underlying co-morbidities that made outcomes a given in many cases.
I can’t come on a public show, but I can share info. My name is Linda (not her real name). In my current position, I read many charts and see in depth info – so much boosting and reboosting and not following other protocols – it’s a given now that the explosions in diagnosis of the cancers and cardiac issues especially come from these decisions. In some cases, the first thing you see on a chart is huge letters stating VAXXED alongside the pt’s diagnosis, treatments thus far, which is usually at odds with normal disease course, age and projected outcome, etc. They’re pushing the vax status, in bright letters, to the top of the list so it can be considered – not for every patient, but the “challenging cases” ... That may be for research purposes.
I will explain the above – what Linda is saying is that practitioners are starting to call out the patient’s vaccination status more clearly on the first screen of the medical record in those cases where they know or suspect the vaccine is related to the patients’s new “mysterious” or “complex” problem. Let’s be clear though, the doctor’s don’t necessarily or explicitly include vaccines as a possible cause in their reasoning/impression/plan section of the patient note. But it seems the nurses and junior docs are now calling it out in some small/large way. Disassociation breaking, ever so slowly?
It makes me just stop, and by end of the week, take into account cases of say, ocular orbital cancer in 20-somethings. Have had 6 in last 2 weeks with no Family History or other indicators. Out of the blue, some with brain mets now. All vaxxed unwillingly, all had Covid and recovered fine prior to employer forced vax. The employers, the areas the patients reside in….nothing in common other than the previous. The actuaries are correct. Excess mortality, let along whatever-life-left disability. Stunning numbers.
I ended up talking to Linda… about lots of things. She is clearly a fellow spirit, highly experienced in ICU and Emergency medicine, and she told me even more disturbing developments, like the fact that on some night shifts, nurse teams are seeing more cardiac arrests in a single shift than ever before and in unprecedented younger age patients. On some shifts, they have had so many that the “crash carts” are rolled straight from one arrest to another because Pharmacy, especially on night shifts, are not able to re-stock fast enough. This situation has happened maybe once in my whole career… when two arrests happened on the same floor or unit within a short time period.
She also told me that night nurses are more openly discussing the vaccine as the cause of what they are seeing (much more than during day shifts apparently). However, they do this largely in text, and they use “code”. Their code word for a vaccination injury or cause is “that issue,” i.e. in reference to a 22 year old who suddenly arrested on the hospital ward, “he is having that issue.” Note these are nurses.. not the docs.. but some of the docs are talking to her, like the one above who performed 6 enucleations (eyeball removals) this year already in young people (very rare to have to do this, especially in this age group). She also told me about how her interventional cardiologist nurse friends related that some patients are coming in with massive heart attacks, and during the angiogram the interventional cardiologists are seeing such extensive thrombi filling the entire artery (as documented by some embalmers), that they say “I can’t stent or remove this, this guy needs surgery, like now.”
In that conversation with Linda, I was also finally able to confirm a fraud that I had suspected was occurring within U.S hospitals regarding the accuracy (or willful inaccuracy) of the vaccination status listed in the medical record of a patient newly admitted to the hospital. It has long been my strong belief that this fraud drove the U.S data used to support some of the last remaining false narratives (i.e narratives #6 and #7 below) . Note these ever-shifting narratives were all directed at combatting vaccine hesitancy, which as some of you may know, was the primary military objective of the vaccinators.
BMGF/WHO/NIH et al. had clearly identified vaccine hesitancy as the main enemy in the battle plans they drew up and distributed after their viral pandemic simulation exercises over the past decade. In this prominent medical journal publication on addressing viral pandemics, they state “the World Health Organization has listed vaccine hesitancy among the greatest threats to global health, calling for research to identify the factors associated with this phenomenon.” Vaccine hesitancy is why the HHS gave $1 Billion to U.S media to support a relentlessly positive public relations campaign supporting the uptake of vaccines.
Now let’s get back to this fraud. First, note that during all of 2021, (well, up until late November when I was let go from my last pandemic ICU job on a completely fabricated accusation), I had only taken care of one ICU patient that was officially documented in their medical record as “fully vaccinated.” I knew that it could simply not be true that only one patient that I took care of the entire year was fully vaccinated. I knew this was false based on data from countries that more transparently (mistakenly?) reported vaccination status and hospital outcomes. In multiple reports starting in February 2021, the majority of hospitalizations and deaths (even when adjusted to rates per 100,000) had long been the vaccinated.
One of the more ridiculous attempts to cover this fraud up in the U.S was a media narrative launched in June/July of 2021, created from statements by Fauci and Walensky, that 99% of patients in hospital and dying were the unvaccinated. They literally did this with a straight face, knowing that they were including in their numerator all the deaths that occurred prior to the start of the vaccination campaign. Yup, if you died in 2020, you were reported as dying in an unvaccinated status. Not subtle. But that was not the only lie. We must never forget the famous slip by the NY times.. when they suddenly and surprisingly called out the CDC for “withholding large amounts of COVID data” throughout the pandemic. Umm.. their actual job is to collect and disseminate data. Not subtle. Even crazier is that at the time of that narrative launch, during a lecture, a CDC slide deck mistakenly showed a slide which revealed that 26% of patients in U.S hospitals were vaccinated. But this number was falsely and fraudulently lower than the actual number. By a long shot.
Here is how I think they falsely suppressed the real rate of vaccinated patients entering U.S hospitals and dying:
In the most popular electronic medical record system in the U.S (EPIC), on the sidebar of every page in the chart are the name, demographics, room number, provider team, and COVID vaccination status of the patient. What I found weird from the outset was that, in EPIC, there were only two categories under the COVID-19 vaccine status section, “Vaccinated” or “Unknown.” There was no “Unvaccinated” status. Also realize that “Unknown” was interpreted by all providers and official data as akin to being “Unvaccinated”. Everyone I took care of in the ICU in 2021, except one, had an “Unknown” vaccination status. How could that be? How come only one ICU patient of mine in the entire year was reported as being “fully vaccinated?” Even if the vaccines worked really well (which I knew they didn’t), something was off, like really off.
There was only one hypothesis I could come up with to reconcile these observations. I suspected that during the admission process to the hospital, there must have been some sort of barrier to deeming someone “vaccinated.” I hypothesized that in order to be documented as vaccinated on admission, you had to have received the vaccine from a primary care physician’s clinic who worked for that same hospital system in a system office, and that they had already documented in the electronic medical record. If you got a vaccine from anywhere else outside that hospital system’s clinic, you were assigned an “Unknown”, i.e. “Unvaccinated” status in the electronic medical record.
And lo and behold, Linda confirmed this was the case in one major health system she worked at. What I found most striking is that she worked in two different hospital systems, in one (the smaller one) it was very easy to document a patient in the record as vaccinated. The admitting nurse could accept any documentation, from a Walgreen’s card to even a verbal report from the patient or family and they could put it in the record on admission and the patient would show up as “vaccinated” on the main screen sidebar.
In the other, larger, major (and I mean major) health system she worked in, if the patient received the vaccine from anywhere but an employed provider’s clinic within the health system (even if the patient had a vaccine card on them), she was forced to put it in an “open field” buried on page 2 of the initial nursing assessment where nobody, and certainly no physician looked for it. All these patients were automatically documented on the main screen as “Unknown”, i.e “Unvaccinated”, even if the dates of each shot were entered into that nursing note field.
This process is what led the vast majority of U.S doctors to become convinced that the only people dying in hospitals were the unvaccinated. Which made perfect sense, I mean, the vaccinators did not want anyone to know the vaccines were not preventing hospital or death, so it would be helpful to their mission if they could make everyone think that all hospital patients were unvaccinated. This way, all the health care workers would get vaccinated out of fear of dying and would also aggressively insist that all their patients and family members get vaccinated. Which is what happened. It is also why a large percentage of the population (at least the ones I meet at lectures, conferences, and symposia) no longer want to see a “system doctor” or go to a “system hospital,” no matter how grand their brand/reputation once was. Fun fact: a long-time donor of large annual gifts to the Mayo Clinic.. decided to direct their donation to the FLCCC this year because they felt the Mayo Clinic had departed from their founding principles and mission. Go FLCCC.
The system docs behaved this way because they saw with their own eyes “the (false) reality” of what would happen if you were unvaccinated. This, combined with the medical journal propaganda publishing only favorable and selective analyses of vaccine efficacy and safety drove nearly all the nation’s doctors to go completely mad.
Their fervor to vaccinate everyone and everything, even in patients who just recovered from COVID, was something to behold. I saw overt hectoring, harassment and even rage. Twitter was one of the most terrifying places to watch doctors arrogantly propagate the need to be vaccinated.. even for folks who had (often hard-earned) natural immunity. I almost feel bad for some of those docs as history will not judge them kindly. Forgive them for they know not what they do. They were literally screaming across Social Media, Media, and Medical Journal editorials, that you will be OK if you just get vaccinated. The high profile docs were the worst, except I have little sympathy for them as some/many/most were likely complicit in the deception rather than just fooled like the rest. Folks like Eric Topol, Peter Hotez, Alastair McAlpine, Tom Friedan (who I used to deeply admire as NYC Health Department Commissioner), Eric Feigl-Ding-(bat), Jeremy Faust (probably the biggest ignoramus on Twitter, having taken an early lead in that competition since the pandemic broke in 2020), and Monica Gandhi. Leana Wen deserves particular ire as she is the most active prostitute for the Pharma-captured federal health agencies on mass media. A media darling as it were.
Then you started to see doctor walk-outs protesting the unvaccinated, increasing numbers of doctors publicly stating they would start refusing to see unvaccinated patients, heck, the Pharma controlled outlet called Medscape even got an ethicist to argue that it was OK to refuse to treat the unvaccinated. Yup. Crazy town. Clown World. One of my patients who is a hospital pharmacist even told me that at her hospital, the hospitalists were vaccinating patients admitted for COVID..as they were being discharged from the hospital. That’s right, as the patients were being discharged after having recovered from COVID, they were recommending and administering vaccines for the same illness. I even heard of one case where a team of clinicians decided to vaccinate a severely ill COVID patient in the ICU.
I also witnessed aggressive attacks in one of the nation’s largest medical-centers staff physician email forum. Doctors “screaming” that everything would be fine if everyone just got the damn vaccine. Deriding anyone bringing forth arguments about untested safety, suspicious efficacy data, and concerns about mandates violating patient autonomy and medical ethics. Anyone who brought forth “adverse data” towards the vaccines were treated with dismissal and a retaliatory posting of selectively favorable data with the imprimatur of the Pharma captured agencies and Pharma captured journals. I will never forget this time in the history of medicine. Ever.
Some other “insights” into the medical system I haver come across, from another ER nurse:
I have no research to offer but first hand experience from working as an RN
in an ER.Ringing in ears and hallucinations have followed vaccinations in 3 of my
patients. Family members at a loss. I mention the vaccine but most don’t
even hear it……..The gentleman with the ringing in the ears (just had his 4th booster the day
before) I suggested he didn’t get any more boosters as ringing in the ears
is an adverse reaction to the vaccine. His wife looked at me and yelled
“his doctor told him he won’t survive the anti-virals for COVID” I was
speechless. The patient continued on and told me about his experience with
the vaccines 1st shot-he had a seizure, doctor recommended 2nd shot. After
2nd shot he was very sick, doctor recommended 3rd shot and he was
hospitalized 4th shot ringing in ears, abdominal bloating and months away
from dialysis. Wife added that he also had seizure after first vaccine and
she had that attitude that it was no big deal.I have said this before, it’s criminal what is happening. I have cried on
my way home from shifts, I tell whoever will listen. The information I have
collected over the last 7 months (time of vaccine/booster in relation to
chief complaint) is jaw dropping.I took a break from working for the summer but continue to keep in touch
with the nurses……My friend told me about an 80yr old man, 4 strokes in the last year and
they all line up with his 4 shots but the doctors response is “he’s 80,
he’s going to have strokes”Has anyone come across research in regards to GI bleeds and low hgb? I have
a lot of this patients, GI bleeds out of the blue…….and they are young!I had 28yr old black obese young woman…..new diagnosis of enlarged heart
and CHF. Vaccine was roughly 1 month prior to ER admit and I suggested no
more vaccines for COViD and her response was “my doctor told me this
happened because I got the vaccine and a tattoo on the same day”60ish lady…….just got over COViD (after have 3 COViD vaccines) and she told
me she was going in for second booster next week!!!!!!Kids are having random seizures and are put on anti-seizure medication for
2 years…when I ask parents what caused the seizure, the neurologist has no
idea. All these children vaccinated for COViD-100%. NO ONE CONNECTS THE
DOTS.The screenshot below is of 3 days I worked and I’m in the ER for 12 hours
and don’t see all admits. I’m also super busy so it’s hard to check status
of all admit patients……of course this is very limited information but a lot
of the patients have some issue 2-3 months post vaccine/booster.
I’m still shocked we don’t have a “vaccine team” monitoring all the
patients as they come into the ER but no one cares. Not the ER medical
director, not the doctors, not the COViD response team…..no one. Nurses see
it and they are talking but many are fearful of getting fired.Thank you for all that you are doing! Although I can’t read all the emails,
I am just happy to know that there are others out there that are in the
same boat as I am.I’m disgusted with the AMA and AAP. I don’t trust a thing they say. I don’t
trust them with my four children as they have not protected our children
over the past 2 years.Thank you!
And another:
May 26 05:28PM -0400
Katie (not her real name),
Thank you for sharing your story! This is what I live every day and I tell my husband how hard it is to see so much damage. I have had more patients diagnosed with aggressive cancers than I have seen in the last two decades.…I’ve been so especially concerned about the clotting effects with Total joints treated with Tranexamic Acid. I’ve been keeping track of my patients (that I would consider) have had mild/moderate vax injury. i.e. – reactivation of latent viruses, (oral herpes (not just one or two lesions, but their whole mouth broke out – something that had never happened before) shingles – affecting their eyes, that took more treatment than normal) – Histoplasmosis; *blood clots/Cardiac problems – Stroke from new onset Atrial fib in a patient on blood thinners within 12 hr post injection, Atrial fibrillation in a healthy, athletic 34 yr old male, new onset hypertension without prior history; * Persistent cough, months of diarrhea, migraine, neuropathy of upper extremity to the extent she could not write/type – all extensively checked out without cause. But, all within a few days/weeks/couple months of injection. All my practitioners are still advocating the Vax!!! What do you think we should do??? I’ve got to get the guts to gently visit with our Chief of Staff. CRNA, Colorado
Last one, from a colleague:
Just had dinner with my friend, a colleague friend of his here, Dr XXX renowned YY Physician . PRO Vaccine. Was adamant all physicians should get the vaccine and should not be able to practice without it. Was a trailblazer for the vaccine here. He got boosted around Christmas time, had a stroke less than a week after, lost his eyesight in one eye, lost his practice, cannot be a doctor any longer, and said undoubtedly it was from the Pfizer vaccine and encouraged all of his doctor friends to max out their disability insurance to protect themselves. I know not surprising to you, but this guy was so pro vaccine and clearly admits his stroke and his loss of eyesight from the vaccine!!
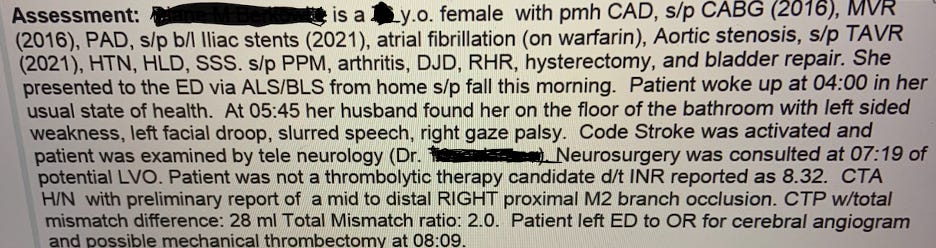
And then there is this doozy – another nurse sent me a case history below of an elderly woman whose blood thinner was highly “supra-therapeutic” (i.e. very thin blood at risk of major bleeding), yet she had a massive stroke caused by a blood clot. This simply does not happen.
El Fin.
I just want to say how much I appreciate all the subscribers to my substack, and especially the paid ones! Your support is so greatly appreciated.
P.S I have recently entered private practice and opened a tele-health clinic providing care not only in the prevention and treatment of acute COVID, but with a specialized focus on the study and treatment of both Long-Haul and Post-Vaccination injury syndromes. If anyone needs our help, feel free to visit our website at www.drpierrekory.com.
P.S.S I am getting professional help (hah!) to write a book about what I have personally witnessed and learned during Pharma’s Historic Disinformation war on ivermectin. Pre-order here for:
************
Source
Published to The Liberty Beacon from EuropeReloaded.com


••••
The Liberty Beacon Project is now expanding at a near exponential rate, and for this we are grateful and excited! But we must also be practical. For 7 years we have not asked for any donations, and have built this project with our own funds as we grew. We are now experiencing ever increasing growing pains due to the large number of websites and projects we represent. So we have just installed donation buttons on our websites and ask that you consider this when you visit them. Nothing is too small. We thank you for all your support and your considerations … (TLB)
••••
Comment Policy: As a privately owned web site, we reserve the right to remove comments that contain spam, advertising, vulgarity, threats of violence, racism, or personal/abusive attacks on other users. This also applies to trolling, the use of more than one alias, or just intentional mischief. Enforcement of this policy is at the discretion of this websites administrators. Repeat offenders may be blocked or permanently banned without prior warning.
••••
Disclaimer: TLB websites contain copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available to our readers under the provisions of “fair use” in an effort to advance a better understanding of political, health, economic and social issues. The material on this site is distributed without profit to those who have expressed a prior interest in receiving it for research and educational purposes. If you wish to use copyrighted material for purposes other than “fair use” you must request permission from the copyright owner.
••••
Disclaimer: The information and opinions shared are for informational purposes only including, but not limited to, text, graphics, images and other material are not intended as medical advice or instruction. Nothing mentioned is intended to be a substitute for professional medical advice, diagnosis or treatment.



Leave a Reply