


ER Editor: English-speaking culture, especially American, has yielded a considerable number of medical whistleblowers from the beginning, and which we have been publishing in order to get at the complex nature of the medical scam that is being conducted against the citizenry during the entire covid plandemic. In France, these lone voices are harder to come by, however. It has taken longer to get at the real situation in France, although it is sounding much like situations we have reported on elsewhere.
This article was written by political scientists, not doctors. We have published extensively on the testing and diagnosis of covid, and what constitutes (or not) a valid ‘case’ and ‘death’ from this alleged virus, enough to bring into doubt all statistics. We have also published much on the dubiousness of vaccines, those in relation to covid and those not. In this article, therefore, we are ignoring those kinds of claims. Instead, our concern is on government policy regarding its medical personnel, the public, and treatments, etc.
In this insightful report, it is clear that the French government has:
- warned patients not to see their family practitioners
- rendered family doctors impotent in what they could prescribe for their patients (nothing, in fact)
- left covid-afflicted patients at large, to be in contact with others; left hospitals and even carehomes to become infection vectors, while not protecting their staff with suitable PPE
- banned the prescription of chloroquine-type medications by family doctors
Suddenly, family doctors have been completely sidelined, in a situation where they would normally be on the frontline. Because … ? Hydroxychloroquine, most probably.
**********
Covid-19 or Influenza A H1N1: France has excluded general practitioners!
What a humiliation to exclude GPs in this way every time there is a pandemic! It is all the more humiliating and serious since no reaction has been recorded from them, and even less from the National Order of Physicians or the trade unions! After 10 years of very difficult studies and knowing one’s patients perfectly well, the government will not have been able to understand that they are the best people to put forward for this health crisis. Except that the executive preferred once again to centralize everything in the public hospital in order to control EVERYTHING and above all to dictate prescriptions and treatments!
(ER: it is our view that, on the contrary, the government knows perfectly well that family doctors know their patients best, which makes sidelining them all the more suspicious.)
*****
MEDIAPART
By Dominique ANDOLFATTO and Dominique LABBÉ
The Covid-19 has so far killed between 30,000 and 40,000 Frenchmen (depending on whether or not one counts the probable number of deaths at home).
With the lack of protective equipment and tests, the main causes of the French hecatomb lie in the demobilisation of general practitioners and the refusal to let them free to practice their profession as doctors.
To date, covid-19 has killed between 30,000 and 40,000 Frenchmen (depending on whether or not one counts the probable number of deaths at home). Compared to other epidemics, this toll is far from being a record (see our previous article on this subject). It nevertheless appears very heavy compared to that of most other countries (see Table 1). According to the data used, France ranks 4th or 6th among the main Western countries in terms of mortality. Only Belgium and the United Kingdom do – unquestionably – less well. Clearly, the health system has been put under strain. Dysfunctions, which we must try to understand, have occurred even if, at the highest levels, complacency now seems to be the order of the day.
Table 1: Comparative assessment of the COVID-19 epidemic in 21 countries

Covid-19: a breakthrough in the fight against epidemics
How can we explain such a level of mortality, which ranks France among the Western examples not to follow in the face of the pandemic? To answer this question, it is first necessary to understand how this type of epidemic is usually dealt with before seeing what has changed in 2020.
The modern fight against epidemics is based on a few simple principles: “protect the weakest – detect the sick – keep them away and care for them”. For two centuries the “general containment” of populations has been abandoned, except when the presence of the infectious agent is still limited to the area where it appeared.
For example, by 2015, seasonal influenza in the northern hemisphere had taken on a disturbing character because the strain was not covered by the vaccine. It was at least as contagious and virulent as SARS-coV-2 in 2019-2020, and no known medication had been proven effective against it. However, no “health emergency” was declared and excess mortality was limited to a level roughly equal to that of covid-19.
During the 9 weeks of this epidemic, there were approximately 3 million medical consultations for influenza-like illness, with 30,911 emergency room visits resulting in 1,597 resuscitations (see data here). Most of the “shock” was therefore absorbed by the general practitioners: they treated 99% of the cases with the usual cocktail: “stay home + antiviral + antibiotic”. In this equation, the first term was the most important: confined at home until no longer contagious, the patient does not infect others, which is the surest way to curb the epidemic. As for the traditional dosage, it helps the immune system work, prevents opportunistic infections and reduces the duration of contagiousness. General practitioners have used the usual diagnosis. Tests were carried out on hospitalized patients and for the surveillance of the nursing staff in hospitals and EPHADs where special asepsis and protection instructions were applied.
Compared to this proven traditional pattern, giving primary care its rightful place, everything was changed in 2020.
One of the keys revealing this change – probably the most important – is to be found in the report of the National Assembly’s fact-finding mission “on the impact, management and consequences” of the epidemic, published on 3 June, 2020. This report preceded the work of the commission of inquiry that opened on 16 June but, curiously, it left the media indifferent. However, the parliamentarians provided – perhaps without really realizing it – a decisive piece of information: the table at the bottom of page 79 of their report.
A double break
The first three lines of Table 2, below, are taken from this parliamentary report. We add the number of hospitalizations for covid-19 (published by SPF) and calculate the proportion of cases of covid-19 treated in emergency (last line).
Table 2: Number of consultations for suspicion of covid-19 (with general practitioners, SOS-medecins* and in the emergency room) and number of hospitalisations (classification by week)
*ER: SOS-medecins is an emergency service you can call to have a doctor, not your family physician, make a house call.

It should be remembered that in 2015 (and, in fact, in every seasonal epidemic before 2020), city medicine (ER: the family doctor) treated 99% of lung infections and the hospital system treated only the 1% most serious ones requiring intensive care. On the other hand, in that year, as usual, about one death in two occurred at home, either because the patient or his or her family refused to be transferred to hospital or because the physician felt that the patient’s age and general condition did not warrant a final rescue attempt. After all, this “end-of-life support” function was also part of the traditional functions of the “family doctor”, a function that was de facto abolished in 2020 for most covid-19 patients.
Indeed, for this epidemic, the last column of the table indicates that there would have been :
– ten times fewer consultations in town (general practitioners + SOS doctors) than before for this kind of epidemic (247,000 instead of about 3 million);
– more than a third of patients ended up in hospital (compared to about 1% before 2020);
– from 30 March onwards – when the peak of the epidemic had not yet been reached – a sharp drop in the number of consultations among GPs.
ER: Doctors in France are a ‘liberal profession’ meaning they get paid a set sum for each patient visit; they are not on a government salary. Thus, their incomes would have declined considerably during this time unless they could skype with patients. Even then, it would not have made up for a dramatic loss in patient footfall.
The doctors were alarmed by this. In a press release of 27 March 2020, the general practitioners’ union MG France denounced for example the Prime Minister (ER: former PM Edouard Philippe), who “dissuades patients from going to see their doctor, by explaining in an authoritative manner that going to see one’s doctor is more dangerous than going to buy a baguette of bread or a packet of cigarettes”. Between 5 and 12 April there is still a tenfold division in the number of consultations, and SOS-médecins takes care of more patients than all the other French GPs combined! Graph 1, below, illustrates the extent of the phenomenon.
Graph 1: Number of consultations at GPs and in emergency departments compared to hospitalisations
ER: The sharply rising and then steeply declining black line shows the number of family doctor consultations. Lockdown started on March 16.
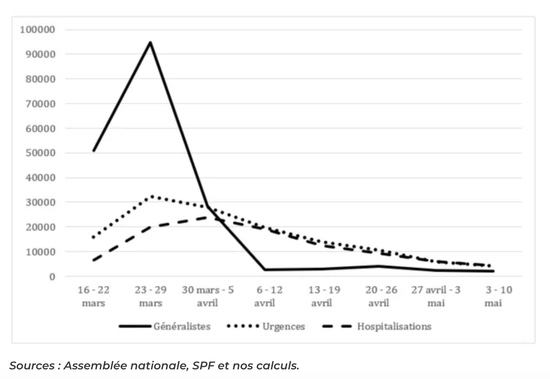
During the first two weeks of confinement, all three curves move in the same direction. The strongest growth is seen among general practitioners. Admittedly, the ratio between the number of emergencies and consultations among GPs is only one to three, whereas for influenza, it was more like 1 to 100. From the outset, the contribution of GPs seems modest, as if a large proportion of doctors had taken a back seat.
Normally, the three curves should have the same profile. The peaks in consultations and emergencies should have been between April 1 (maximum number of new hospitalizations), April 8 (peak of people in intensive care) and April 14 (maximum number of people in hospital). However, from the end of March, while the epidemic was still growing, a double break (ER: change) occurred.
The first break was in the emergency room. From the week of March 23rd, the curve of the emergency visits is close to that of hospitalizations and merges with it from April 6th. This is an unprecedented situation. Usually, a part of the patients who arrive at the emergency rooms of the hospitals leave, after examination and care if necessary, without being hospitalized. Three explanations are cumulative.
Firstly, it can be assumed that patients who presented spontaneously – because they thought they had the symptoms of the disease and were unable to get an appointment with their GP – were either hospitalized because their condition was critical, or sent home and to use the emergency number if their condition worsened. This referral would have been made without the patient having been examined by a doctor as is customary (and would therefore not have been counted).
Second, the emergency services screened severely and only took care of the most serious cases. This triage would have been done over the telephone, since when the EMS is on the road, this intervention is counted as such.
Finally, and most importantly, according to government instructions widely disseminated in the media, most of the patients probably waited until they were in great difficulty to call the emergency services. On various blogs and social networks, there are many complaints about the difficulty of reaching this number, sometimes for days on end.
As a result, the number of deaths at home may be higher than the 9,000 estimate mentioned at the beginning of this article. In any case, this is an unprecedented situation in recent health history.
The second break is spectacular. The number of consultations at GPs collapses and falls below the number of hospitalizations. From the week of April 6, it falls to 2,663 (35 times less than 2 weeks earlier), while the epidemic is at its peak.
What events could have led to a low number of GP consultations from the very beginning of the epidemic, and then such a spectacular – and to our knowledge, totally unprecedented – withdrawal on the part of general practitioners?
Was primary care banned?
On March 14, the High Council of Public Health (HCSP) recommended to general practitioners to use only paracetamol to the exclusion of any other drug. This is the first time in our history that doctors have been told not to prescribe… not to prescribe.
On the same day, in its first opinion, the Scientific Council, charged with enlightening the President of the Republic, justified the decision to close schools and confine the population by the statement “in the absence of treatment and vaccine”.
On 23 March, the same scientific council made the following recommendations to general practitioners:
“The detection and management of patients with COVID-19 should be carried out as far as possible by avoiding the visit of these patients to the doctor’s office (…) When a consultation in the doctor’s office is deemed essential by the general practitioner, it will be carried out at dedicated times to avoid contact with other uninfected patients, will be carried out with the necessary protective equipment, and will be followed by appropriate disinfection measures. Patients must be transported to and from the practice in a safe manner. If the physician goes to the patient’s home, the same recommendations apply.”
It should be remembered that, at the time, protective equipment (masks, gloves, over-blouses, etc.) was totally lacking and that, compared to the cost of the consultation (ER: around 25 euros per visit), these recommendations seem very difficult to implement.
On March 25, a decree of the Ministry of Health reserves the prescription of quinine derivatives (ER: chloroquine is a semi-synthetic quinine derivative) to hospital establishments. Private doctors are no longer authorized to prescribe it, and then on March 26, the ANSM (National Agency for the Safety of Medicines) banned pharmacists from dispensing these drugs except in the case of certain pathologies (HIV, lupus, rheumatoid arthritis).
On 27 March, the Scientific Council of the National College of Teaching General Practitioners (CENG) recommended that general practitioners should not prescribe quinine derivatives for the treatment of covid-19. It added that “this prescription would be contrary to medical ethics”. This formula has a specific practical meaning: any physician who violates the deontology of his profession may be suspended immediately by the Council of the College. On the same day, the National Council of the College of Physicians and Surgeons resumed these injunctions, giving them the force of law.
The statistics unveiled by the National Assembly’s commission of inquiry, summarised in Table 2 and Graph 1, above, clearly show that, less than a week after these injunctions, the overwhelming majority of GPs had complied by closing their doors to patients with covid-19 symptoms, refusing home visits and advising only to take paracetamol (over-the-counter and therefore not requiring a consultation) and to go to the emergency room in the event of aggravation. Until 10 May – the date of the last published data – they did not change this attitude.
These patients had two ultimate recourses: SOS-physicians and the emergency department. However, from the week of March 30, which followed these injunctions, and while the disease is still spreading, SOS-medecins consultations are also declining (they should have exploded since the general practitioners have closed their doors). The emergency room is reserved for patients in critical condition brought in by the emergency services.
Some doctors have persisted in wanting to care for and treat their patients using the available pharmacopoeia, and not only paracetamol, which, moreover, is not without perverse effects. Then, on April 23, the Council of the Order became more threatening. He reiterated the prohibition of any attempt at treatment that was in fact an experiment – since, in his opinion, the disease was new and without admitted treatment. Consequently, any treatment had to obey a cumbersome and complex procedure (declaration to the ANSM) and, in fact, was doomed to failure in the case of private doctors. This could only end up depriving doctors of any means in the face of a rapidly and strongly growing epidemic.
Some of them still persist, notably by resorting to antibiotics to fight the disease, the HCSP, following the recommendations of the ANSM and the Directorate General for Health, advised against the use of these drugs (see the reactions of doctors for example here). At the same time, at the beginning of June, the departmental doctors’ orders announced that they would immediately summon, for explanation, the few doctors who had not respected or would still not respect these “recommendations”.
Dramatic consequences
While France devotes 12% of its national income to health, for the first time in contemporary history, hundreds of thousands of people with social insurance have been refused the access to a doctor, the listening and the care to which they are entitled.
In addition to the psychological drama felt by these people abandoned to their fate, the consequences in terms of public health are obvious and dramatic.
The (ER: covid-suspected) patient remained “in circulation” instead of being confined, contrary to all recommendations and medical practice in the face of epidemics. William Dab, former Director General of Health, cruelly reminded the health authorities of this in an interview with the newspaper Le Monde, unfortunately published two months after the epidemic peak: “We have known since Robert Koch [discoverer of the bacteria responsible for tuberculosis] that the surveillance-test-tracer-isolation sequence is the basis for controlling communicable disease epidemics”. The same man drove home the point by stating that, since the beginning of June, this sequence “is now better implemented”.
During the most intense period of the epidemic, the patient – whose condition was not considered serious enough to be sent to the emergency room by the rescue services – was left to fend for himself. He infected his relatives, shopkeepers and their customers when he went shopping. If he was one of the “requisitioned” workers, because he had not stopped working, he spread the virus in the metro, on the bus, among his colleagues at work, etc. He was then sent to the emergency services. If he was a carer or service staff in a hospital or EPHAD (ER: old people’s care homes), he spread the disease among the people at risk who should have been protected. Thus, “situations of superpropagation” developed, according to another formula of William Dab. (ER: A reminder that no masks were required at this time! Unlike now when the virus is impotent.)
There is nothing theoretical about this perspective. After having long refused to systematically test health workers, it had to be acknowledged that many had contracted the disease: as of 14 May, a partial census indicated that more than 65,800 health and “medico-social” professionals had a symptomatic form of the disease which led to them testing positive. 75% of them were working in EHPAD. Nurses were the most affected. As these personnel were not confined before presenting serious symptoms (since they could not see their general practitioners for a work stoppage – ER: a family doctor’s note is required to legitimately miss a day of work), they each contaminated several “people at risk”. This explains the appalling mortality in the EPHADs.
In the Italian case, a team of doctors from Lombardy clearly analysed this situation as early as 21 March 2020:
“Hospitals could be the main vectors of covid-19, as they were quickly populated with infected patients, which facilitates transmission to uninfected patients. Patients are transported through our regional system, which also contributes to the spread of the disease as its ambulances and staff quickly become vectors. Health workers are asymptomatic or unattended sick carriers”.
Conclusion: the strange defeat
The very harsh and undifferentiated confinement of the entire population has been unnecessary and the whole society has been affected. With the lack of protective equipment and tests, the main causes of the French hecatomb lie in the demobilisation of general practitioners and the refusal to allow them to exercise their profession as doctors.
This debacle calls into question a highly centralised health organisation, the public authorities’ contempt for GPs, the State’s lack of confidence in civil society, and also the economic model of the pharmaceutical industry, whose existence depends on the rapid replacement of existing medicines by new products with often questionable efficacy.
Last but not least, this policy, in addition to failing to prevent a significant excess of deaths, led to a democratic regression – favouring for several weeks a surveillance and punishment society – and then to the most serious economic crisis since the 1930s and the Second World War. The number of unemployed people is increasing dramatically while the deficit of Social Security – and more broadly of the welfare state – has become abyssal, as never before.
By Dominique ANDOLFATTO (Professor of Political Science, Credespo, University of Bourgogne Franche-Comté) and Dominique LABBÉ (Associate Researcher in Political Science, Pacte-CNRS, University of Grenoble-Alpes).
LAURENT MUCCHIELLI
Mediapart [LAURENT MUCCHIELLI’S BLOG]
***********
Original article
Published to The Liberty Beacon from EuropeReloaded.com


••••
The Liberty Beacon Project is now expanding at a near exponential rate, and for this we are grateful and excited! But we must also be practical. For 7 years we have not asked for any donations, and have built this project with our own funds as we grew. We are now experiencing ever increasing growing pains due to the large number of websites and projects we represent. So we have just installed donation buttons on our websites and ask that you consider this when you visit them. Nothing is too small. We thank you for all your support and your considerations … (TLB)
••••
Comment Policy: As a privately owned web site, we reserve the right to remove comments that contain spam, advertising, vulgarity, threats of violence, racism, or personal/abusive attacks on other users. This also applies to trolling, the use of more than one alias, or just intentional mischief. Enforcement of this policy is at the discretion of this websites administrators. Repeat offenders may be blocked or permanently banned without prior warning.
••••
Disclaimer: TLB websites contain copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available to our readers under the provisions of “fair use” in an effort to advance a better understanding of political, health, economic and social issues. The material on this site is distributed without profit to those who have expressed a prior interest in receiving it for research and educational purposes. If you wish to use copyrighted material for purposes other than “fair use” you must request permission from the copyright owner.
••••
Disclaimer: The information and opinions shared are for informational purposes only including, but not limited to, text, graphics, images and other material are not intended as medical advice or instruction. Nothing mentioned is intended to be a substitute for professional medical advice, diagnosis or treatment.



Leave a Reply