


Story at-a-glance
-
According to U.S. Centers for Disease Control and Prevention data, more than 1 million excess deaths — that is, deaths in excess of the historical average — have been recorded since the COVID-19 pandemic began two years ago, and this cannot be explained by COVID-19. Deaths from heart disease, high blood pressure, dementia and many other illnesses rose during that time
-
Across the world, death rates have also risen in tandem with COVID shot administration, with the most-jabbed areas surpassing the least-jabbed in terms of excess mortality and COVID-related deaths
-
According to Walgreens data, during the week of April 19 through 25, 2022, 13% of unvaccinated persons tested positive for COVID. Of those who received two doses five months or more ago, 23.1% tested positive, and of those who received a third dose five months or more ago, the positive rate was 26.3%. So, after the first booster shot (the third dose), people are at greatest risk of testing positive for COVID
-
U.K. government data show the all-cause mortality rate is between 100% and 300% greater among people who got their first COVID shot 21 days or more ago. The risk for all-cause death is also significantly elevated among those who got their second dose at least six months ago, and mildly elevated among those who got their third dose less than 21 days ago. As of January 2022, all who got one or more doses at least 21 days ago were dying at significantly elevated rates
-
Other data also show that COVID mortality rates are far higher in areas with high vaccination rates, and risk-benefit analyses reveal the jabs do more harm than good in most age groups
••••
••••
Does the COVID Jab Kill More People Than It Saves?
Analysis by Dr. Joseph Mercola
According to U.S. Centers for Disease Control and Prevention data,1 more than 1 million excess deaths — that is, deaths in excess of the historical average — have been recorded since the COVID-19 pandemic began two years ago, and this cannot be explained by COVID-19.
Deaths from heart disease, high blood pressure, dementia and many other illnesses rose during that time.2 “We’ve never seen anything like it,” Robert Anderson, CDC’s head of mortality statistics, told The Washington Post in mid-February 2022.3
According to University of Warwick researchers, “the scale of excess non-COVID deaths is large enough for it to be seen as its own pandemic.”4 A number of explanations have been offered, including the fact that lockdowns and other COVID restrictions discouraged or prevented people from seeking care. But another, less discussed factor may also be at play.
Across the world, death rates have risen in tandem with COVID shot administration, with the most-jabbed areas surpassing the least-jabbed in terms of excess mortality and COVID-related deaths. This flies in the face of official claims that the shots prevent severe COVID infection and lower your risk of death, be it from COVID or all causes.5
Boosted? You’re Now at Highest Risk of COVID
Ever since the announcement that the COVID “vaccines” would be using novel mRNA gene transfer technology, I and many others have warned that this appears to be a very bad idea.
Numerous potential mechanisms for harm have been identified and detailed in previous articles, and we’re now seeing some of our worst fears come to bear. “Fully vaccinated” individuals are both more likely to be infected with SARS-CoV-2 and more likely to die, whether from COVID or some other cause.
As reported by investigative journalist Jeffrey Jaxen in the April 22, 2022, Highwire video above, data from Walgreens’ COVID-19 tracker6 reveal that COVID-jabbed individuals are testing positive for COVID at higher rates than the unjabbed. What’s more, people who got their last shot five months or more ago have the highest risk.
As you can see in the screenshot below, during the week of April 19 through 25, 2022, 13% of unvaccinated tested positive for COVID (with Omicron being the predominant variant). (The data reviewed by Jaxen are from the week of April 10 through 16.)
Of those who received two doses five months or more ago, 23.1% tested positive, and of those who received a third dose five months or more ago, the positive rate was 26.3%. So, after the first booster shot (the third dose), people are at greatest risk of testing positive for COVID.

A deeper dive into the data7 reveals that two doses appear to have been protective for a short while, but after five months, it becomes net harmful. The group faring worst of all is the 12 to 17 cohort, where no one with one dose tested positive, but after the second dose, cases suddenly appear, and get higher still after five months. After the third dose, positive cases drop a bit, but then shoot up higher than ever after five months.8
Deaths by Vaccination Status in the UK
Data sets from the U.K. government reveal an equally disturbing trend. The raw data from the Office for National Statistics9 is difficult to interpret, so Jaxen had data analysts create a bar graph to better illustrate what the data actually tell us. A screenshot from Jaxen’s report is below.
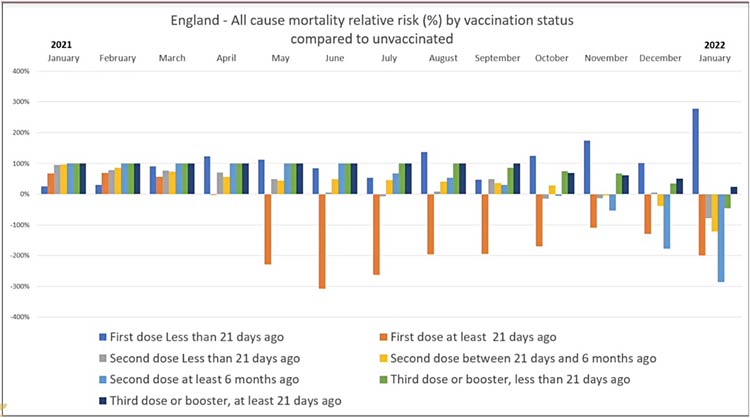
Bars going upward are a good thing, as it indicates the risk for all-cause mortality based on vaccination status is either normal or reduced. Bars that dip below zero percent are indicative of increased all-cause mortality, based on vaccination status.
As you can see, the all-cause mortality rate is between 100% and 300% greater among people who got their first dose 21 days or more ago. The risk for all-cause death is also significantly elevated among those who got their second dose at least six months ago, and mildly elevated among those who got their third dose less than 21 days ago. As of January 2022, all who got one or more doses at least 21 days ago were dying at significantly elevated rates.
More Jabs, More COVID Deaths

Everywhere we look, we find trends showing the COVID shots are resulting in higher death rates. Above is an animated illustration10 from Our World In Data, first showing the vaccination rates of South America, North America, Europe and Africa, from mid-December 2020 through the third week of April 2022, followed by the cumulative confirmed COVID deaths per million in those countries during that same time frame.
Africa has had a consistently low vaccination rate throughout, while North America, Europe and South America all have had rapidly rising vaccination rates. Africa has also had a consistently low COVID mortality rate, although a slight rise began around September 2021. Still, it’s nowhere near the COVID death rates of North America, South America and Europe, all of which saw dramatic increases.
Here’s another one,11 also sourced from Our World In Data, first showing the excess death rate in the U.S. (the cumulative number of deaths from all causes compared to projections based on previous years), between January 26, 2020, and January 30, 2022, followed by an illustration of the tandem rise of vaccine doses administered and the excess mortality rate. It clearly shows that as vaccination rates rose, so did the excess mortality rate.

Risk-Benefit Analysis Condemns the COVID Jabs
At this point, we also have the benefit of more than one risk-benefit analysis, and all show that, with very few exceptions, the COVID jabs do more harm than good. For example, a risk-benefit analysis12 by Stephanie Seneff, Ph.D., and independent researcher Kathy Dopp, published in mid-February 2022, concluded that the COVID jab is deadlier than COVID-19 itself for anyone under the age of 80.
They looked at publicly available official data from the U.S. and U.K. for all age groups, and compared all-cause mortality to the risk of dying from COVID-19. “All age groups under 50 years old are at greater risk of fatality after receiving a COVID-19 inoculation than an unvaccinated person is at risk of a COVID-19 death,” Seneff and Dopp concluded. And for younger adults and children, there’s no benefit, only risk.
“This analysis is conservative,” the authors note, “because it ignores the fact that inoculation-induced adverse events such as thrombosis, myocarditis, Bell’s palsy, and other vaccine-induced injuries can lead to shortened life span.
When one takes into consideration the fact that there is approximately a 90% decrease in risk of COVID-19 death if early treatment is provided to all symptomatic high-risk persons, one can only conclude that mandates of COVID-19 inoculations are ill-advised.
Considering the emergence of antibody-resistant variants like Delta and Omicron, for most age groups COVID-19 vaccine inoculations result in higher death rates than COVID-19 does for the unvaccinated.”
The analysis is also conservative in the sense that it only considers COVID jab fatalities that occur within one month of injection. As demonstrated by the U.K. data above, the risk of all-cause death is nearly 300% greater for those who got a second dose at least six months ago.
Teens Are at Dramatic Risk of Death From the Jabs
Similarly, an analysis13 of data in the U.S. Vaccine Adverse Events Reporting System (VAERS) by researchers Spiro Pantazatos and Herve Seligmann suggests that in those under age 18, the shots only increase the risk of death from COVID, and there’s no point at which the shot can prevent a single COVID death, no matter how many are vaccinated.
“If you’re under 18, you’re 51 times more likely to die from the COVID jab than you are to die from COVID if not vaccinated.“
If you’re under 18, you’re a whopping 51 times more likely to die from the jab than you are to die from COVID if not vaccinated. In the 18 to 29 age range, the shot will kill 16 for every person it saves from dying from COVID, and in the 30 to 39 age range, the expected number of vaccine fatalities to prevent a single COVID death is 15.
Only when you get into the 60 and older categories do the risks between the jab and COVID infection even out. In the 60 to 69 age group, the shot will kill one person for every person it saves from dying of COVID, so it’s a tossup as to whether it might be worth it for any given person.
How Many Are We Willing to Sacrifice?
We also have a risk-benefit analysis by researchers in Germany and The Netherlands. The analysis was initially published June 24, 2021, in the journal Vaccines.14 The paper caused an uproar among the editorial board, with some of them resigning in protest.15 In the end, the journal simply retracted it — a strategy that appears to have become norm.
After a thorough re-review, the paper was republished in the August 2021 issue of Science, Public Health Policy and the Law.16 The analysis found that, “very likely for three deaths prevented by vaccination we will have to accept that about two people die as a consequence of these vaccinations,” the authors wrote in a Letter to the Editor17 of Clinical and Translational Discovery. Defending their work, they went on to note that:18
“The database we based our analysis on was a large naturalistic study of the BioNTech vaccine in Israel. This was the only study at the time that allowed for a direct estimation of an absolute risk reduction (ARR) in mortality.
Admittedly, the ARR estimate was only available for a short observation period of 4 weeks after the first vaccine dose, a point raised by critics. One might have wanted a longer observation period to bring out the benefit of vaccinations more clearly, and our estimate of a number needed to vaccinate (NNV) of 16 000 to prevent one death might have been overly conservative.
The recently published 6-month interim report of the BioNTech-regulatory clinical trial now covers a period long enough to let us look at this risk benefit ratio once again. In Table S4 of this publication, 14 deaths are reported in the placebo group (n = 21 921) and 15 in the vaccination group (n = 21 926).
Among them, two deaths in the placebo-group were attributed to COVID-19, and one in the vaccination group was attributed to COVID-19 pneumonia. This leads to an ARR = 4.56 × 10–5, and conversely to an NNV = 1/ARR = 21 916 to prevent one death by COVID-19. This shows that our original estimate was not so far off the mark.
The most recent safety report of the German Paul Ehrlich Institute (PEI) that covers all reported side effects since the vaccination campaign began (27 December 2020 until 30 November 202119 … reports 0.02 deaths per 1000 BioNTech vaccinations or 2 per 100 000 vaccinations.
We had gleaned four mortality cases per 100 000 vaccinations (all vaccines) from the Dutch pharmacovigilance database LAREB. Using the data of Thomas et al., a liberal NNV = 20 000, we can calculate that by 100 000 vaccinations we save five lives.
Using the PEI pharmacovigilance report for the same product, we see that these 100 000 vaccinations are associated with two deaths, while using the LAREB database back in June 2021, they were associated with four deaths across all vaccines and are associated with two deaths in the most recent reports concerning the BioNTech vaccine … In other words, as we vaccinate 100 000 persons, we might save five lives but risk two to four deaths.”
The risk-benefit ratio may be even worse than that, though, as these calculations do not take into account the fact that passive pharmacovigilance data “are notorious for underestimating casualties and side effects,” the authors note, or the fact that severe side effects such as myocarditis are affecting young males at a staggering rate, which can reduce lifespan in the longer term.
We Do Not Have a Functioning Pharmacovigilance System
In an August 2021 editorial, editor-in-chief of Science, Public Health Policy and the Law, James Lyons-Weiler, Ph.D., wrote:20
“There are two messages from those who hold appointed offices or other influential positions in Public Health on long-term vaccine safety.
The first message is that long-term randomized double-blinded placebo-controlled clinical trials are not necessary for the long-term study of vaccine safety because we have ‘pharmacovigilance’; i.e. long- term post-market safety surveillance that is supported by widely accessible, passive vaccine adverse events tracking systems.
The second message is that any use of those very same vaccine adverse events tracking systems that leads to the inference or conclusion that vaccines might cause serious adverse events or death is unsupported by such systems …
When those seeking support for public health initiatives, such as a new vaccination program, offer evidence that long-term vaccine safety studies are well in hand due to the possibility of detecting adverse events that happened following vaccination, they are either:
(a) unaware that the vaccine adverse events tracking systems upon which they are basing their confidence about society’s ability to detect and track vaccine adverse events are alleged to be unable to be used to infer causal links between health outcomes and vaccination exposure, or:
(b) participating in a disinformation campaign to end scrutiny over the absence of properly controlled long-term randomized clinical trials to assess long- term vaccine safety. Neither of these is sufficient empirical basis for the knowledge claim of long- term safety …
There must be room for disagreement in science; otherwise, science does not exist. It is sad to bear witness to the fact that science has degenerated into a war against unwanted and inconvenient results, conclusions and interpretations via the process of post-publication retraction for issues other than fraud, grave error in execution, and plagiarism.
The weaponization of the process of retraction of scientific studies is well underway, and it induces a bias that could be called “retraction bias”, or, in the case in which a few persons haunt journals in search of studies that cast doubt on their commercial products, a ‘ghouling bias,’ which leads to biased systematic reviews and warped meta-analyses.”
In his editorial, Lyons-Weiler specifically criticized the Vaccine journal for its retraction of the risk-benefit analysis cited above, and mocked the editorial board members who quit in protest, noting that “Rage-quitting is not science.”
“The resigning editorial board members’ knowledge claim is that no deaths have occurred due to the vaccination program. As helpful as that claim might be to a prescribed narrative, it is not based on empirical evidence, and it is, therefore, unwarranted,” Lyons-Weiler wrote.21
“From a Popperian view of science, one can see the fatal flaw in the editorial board members’ knowledge claim: if, as they insist, passive vaccine adverse events tracking systems cannot test the hypothesis of causality, then how can editorial board members, resigning or otherwise, know that the events were NOT caused by the vaccine? …
It is logical to conclude that since passive vaccine adverse event tracking systems do not lend themselves well to testing hypotheses of causality, they do not provide the opportunity to design and conduct sufficiently critical tests of causality, and therefore a replacement system is needed … one that is suitable to detect risk.”
While we may indeed need better pharmacovigilance, there’s really no doubt at this point that the COVID jabs are ill-advised for most people. I believe that in the years to come, people will look back at this time and vow to never repeat it. In the meantime, all we can do is look at and assess the data we do have, and make decisions accordingly.
••••
Sources and References:
- 1 U.S. CDC, Excess Deaths Associated with COVID-19
- 2 MarketWatch February 16, 2022
- 3 The Washington Post February 15, 2022
- 4 Studies in Microeconomics October 19, 2021
- 5 CDC MMWR October 29, 2021; 70(43): 1520-1524
- 6 Walgreens COVID-19 Index
- 7, 8 Bad Cattitude Substack April 15, 2022
- 9 ONS.gov.uk Deaths by Vaccination Status
- 10 Twitter TexasLindsay April 23, 2022
- 11 Twitter TexasLindsay April 25, 2022
- 12 COVID-19 and All-Cause Mortality Data Analysis by Kathy Dopp and Stephanie Seneff (PDF)
- 13 COVID Vaccination and Age-Stratified All-Cause Mortality Risk (PDF)
- 14 Vaccines 2021; 9(7): 693
- 15 Science, Public Health Policy and the Law August 2021; 3: 81-86, page 82
- 16 Science, Public Health Policy and the Law August 2021; 3: 87-89
- 17, 18 Clinical and Translational Discovery February 25, 2022; 2(1): e35
- 19 Paul-Ehrich Institute December 23, 2021
- 20, 21 Science, Public Health Policy and the Law August 2021; 3: 81-86
••••
Dr. Joseph Mercola is the founder of Mercola.com. An osteopathic physician, best-selling author and recipient of multiple awards in the field of natural health, his primary vision is to change the modern health paradigm by providing people with a valuable resource to help them take control of their health.
Theis article (Does the COVID Jab Kill More People Than It Saves?) is republished on TLB with permission and attribution to the author Dr. Joseph Mercola and the website, mercola.com. (© Dr. Joseph Mercola)
This article has been Fact Checked (See fact check statement @ top of article here)
TLB recommends you visit MERCOLA for more great articles and information.
Image Credit: Photo in Featured Image (top) – by nts01 from Pixabay
••••
Read more articles from Mercola
••••
Click on image below to visit site:

••••

••••
Stay tuned to …

••••
The Liberty Beacon Project is now expanding at a near exponential rate, and for this we are grateful and excited! But we must also be practical. For 7 years we have not asked for any donations, and have built this project with our own funds as we grew. We are now experiencing ever increasing growing pains due to the large number of websites and projects we represent. So we have just installed donation buttons on our websites and ask that you consider this when you visit them. Nothing is too small. We thank you for all your support and your considerations … (TLB)
••••
Comment Policy: As a privately owned web site, we reserve the right to remove comments that contain spam, advertising, vulgarity, threats of violence, racism, or personal/abusive attacks on other users. This also applies to trolling, the use of more than one alias, or just intentional mischief. Enforcement of this policy is at the discretion of this websites administrators. Repeat offenders may be blocked or permanently banned without prior warning.
••••
Disclaimer: TLB websites contain copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available to our readers under the provisions of “fair use” in an effort to advance a better understanding of political, health, economic and social issues. The material on this site is distributed without profit to those who have expressed a prior interest in receiving it for research and educational purposes. If you wish to use copyrighted material for purposes other than “fair use” you must request permission from the copyright owner.
••••
Disclaimer: The information and opinions shared are for informational purposes only including, but not limited to, text, graphics, images and other material are not intended as medical advice or instruction. Nothing mentioned is intended to be a substitute for professional medical advice, diagnosis or treatment.


••••
••••